

Report of a phase II study of clofarabine and cytarabine in de novo and relapsed and refractory AML patients and in selected elderly patients at high risk for anthracycline toxicity
- PMID: 21273514
- PMCID: PMC3228084
- DOI: 10.1634/theoncologist.2010-0220
Report of a phase II study of clofarabine and cytarabine in de novo and relapsed and refractory AML patients and in selected elderly patients at high risk for anthracycline toxicity
Abstract
Purpose: To determine the efficacy and safety of clofarabine and cytarabine (Ara-C) in adult patients with relapsed or refractory acute myeloid leukemia (AML) and in elderly patients with untreated AML and heart disease.
Patients and methods: Patients with relapsed/refractory AML and older patients for whom there was a concern over toxicity from additional anthracyclines received 5 days of clofarabine, 40 mg/m(2) per day i.v. over 1 hour, followed 4 hours later by Ara-C, 1,000 mg/m(2) per day i.v. over 2 hours.
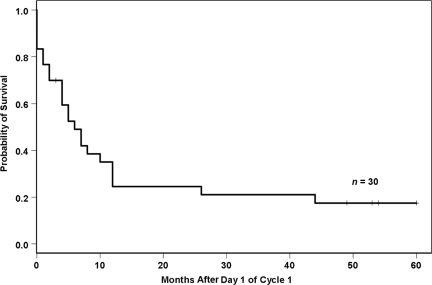
Results: Thirty patients were enrolled. The median age was 67 years (range, 38-82 years) and 18 (60%) had received at least one prior therapy. Eleven (37%) patients had a history of cardiovascular disease and were considered to be at high risk for anthracycline toxicity. High-risk cytogenetic abnormalities were present in 14 (47%) patients. The overall response rate (complete remission [CR] plus partial remission) was 53%, including a CR in 14 patients (47%). Responses were observed in all cytogenetic risk groups and in patients who had received up to five prior therapies. The median disease-free survival interval was 9.5 months. The 30-day mortality rate was 20% (de novo AML, 8%; relapsed/refractory AML, 28%). Of the 14 patients achieving a CR, half were able to proceed to curative hematopoietic stem cell transplantation.
Conclusions: Clofarabine in combination with Ara-C is effective in both untreated and previously treated patients with AML. In addition, it represents a useful remission induction strategy to serve as a bridge to transplantation in older patients with AML.
Conflict of interest statement
The article discusses unlabeled, investigational, or alternative use(s) of a product, device, or technique: Clofarabine is not approved for the treatment of AML in adults (either de novo AML or relapsed/refractory AML), although the results of the CLASSIC I trial in relapsed/refractory AML are anticipated soon.
The content of this article has been reviewed by independent peer reviewers to ensure that it is balanced, objective, and free from commercial bias. No financial relationships relevant to the content of this article have been disclosed by the independent peer reviewers.
References
-
- Horner MJ, Ries LAG, Krapcho M, et al. SEER Cancer Statistics Review. National Cancer Institute: Bethesda, MD; 1975–2006. [accessed March 1, 2010]. Available at http://seer.cancer.gov/csr/1975_2006/ Based on November 2008 SEER data submission, posted to the SEER web site 2009.
-
- Pinto A, Zagonel V, Ferrara F. Acute myeloid leukemia in the elderly: Biology and therapeutic strategies. Crit Rev Oncol Hematol. 2001;39:275–287. - PubMed
-
- Grimwade D, Walker H, Oliver F, et al. The importance of diagnostic cytogenetics on outcome in AML: Analysis of 1,612 patients entered into the MRC AML 10 trial. The Medical Research Council Adult and Children's Leukaemia Working Parties. Blood. 1998;92:2322–2333. - PubMed
-
- Slovak ML, Kopecky KJ, Cassileth PA, et al. Karyotypic analysis predicts outcome of preremission and postremission therapy in adult acute myeloid leukemia: A Southwest Oncology Group/Eastern Cooperative Oncology Group study. Blood. 2000;96:4075–4083. - PubMed
-
- Byrd JC, Mrózek K, Dodge RK, et al. Pretreatment cytogenetic abnormalities are predictive of induction success, cumulative incidence of relapse, and overall survival in adult patients with de novo acute myeloid leukemia: Results from Cancer and Leukemia Group B (CALGB 8461) Blood. 2002;100:4325–4336. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
