

Early postnatal hypotension is not associated with indicators of white matter damage or cerebral palsy in extremely low gestational age newborns
- PMID: 21273984
- PMCID: PMC3145830
- DOI: 10.1038/jp.2010.201
Early postnatal hypotension is not associated with indicators of white matter damage or cerebral palsy in extremely low gestational age newborns
Abstract
Objective: To evaluate, in extremely low gestational age newborns (ELGANs), relationships between indicators of early postnatal hypotension and cranial ultrasound indicators of cerebral white matter damage imaged in the nursery and cerebral palsy diagnoses at 24 months follow-up.
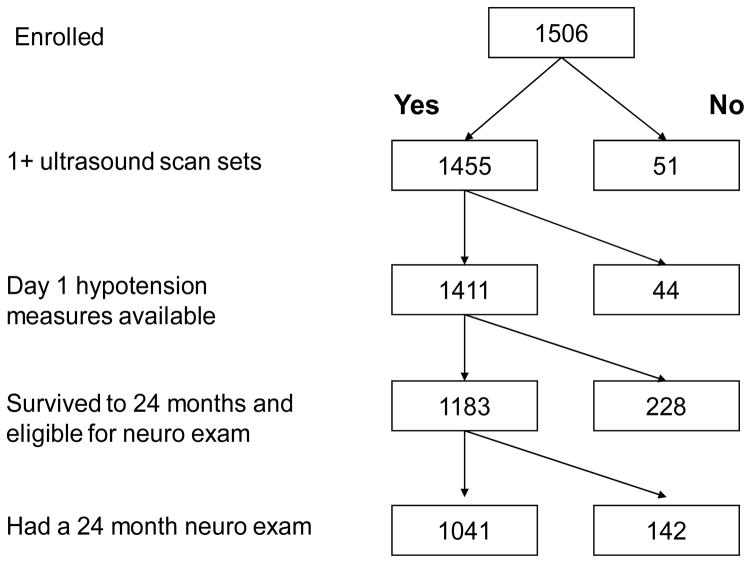
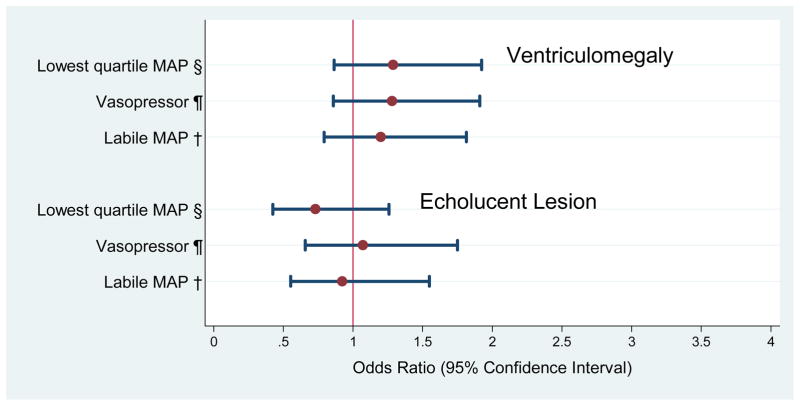
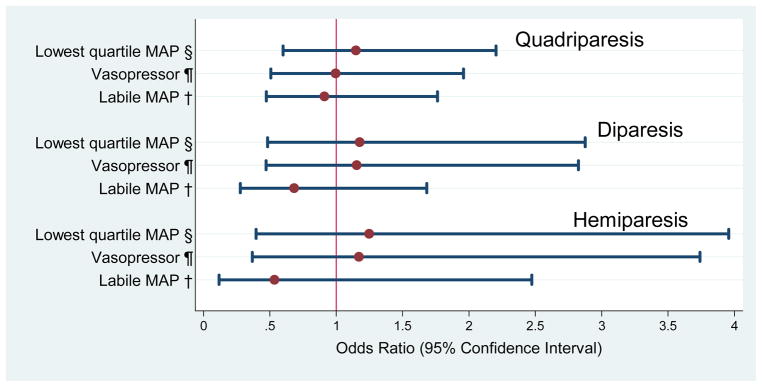
Study design: The 1041 infants in this prospective study were born at <28 weeks gestation, were assessed for three indicators of hypotension in the first 24 postnatal hours, had at least one set of protocol cranial ultrasound scans and were evaluated with a structured neurological exam at 24 months corrected age. Indicators of hypotension included: (1) lowest mean arterial pressure (MAP) in the lowest quartile for gestational age; (2) treatment with a vasopressor; and (3) blood pressure lability, defined as the upper quartile of the difference between each infant's lowest and highest MAP. Outcomes included indicators of cerebral white matter damage, that is, moderate/severe ventriculomegaly or an echolucent lesion on cranial ultrasound and cerebral palsy diagnoses at 24 months gestation. Logistic regression was used to evaluate relationships among hypotension indicators and outcomes, adjusting for potential confounders.
Result: Twenty-one percent of surviving infants had a lowest blood pressure in the lowest quartile for gestational age, 24% were treated with vasopressors and 24% had labile blood pressure. Among infants with these hypotension indicators, 10% percent developed ventriculomegaly and 7% developed an echolucent lesion. At 24 months follow-up, 6% had developed quadriparesis, 4% diparesis and 2% hemiparesis. After adjusting for confounders, we found no association between indicators of hypotension, and indicators of cerebral white matter damage or a cerebral palsy diagnosis.
Conclusion: The absence of an association between indicators of hypotension and cerebral white matter damage and or cerebral palsy suggests that early hypotension may not be important in the pathogenesis of brain injury in ELGANs.
Conflict of interest statement
This study was supported by a cooperative agreement with the National Institute of Neurological Disorders and Stroke (5U01NS040069-05) and a program project grant from the National Institute of Child Health and Human Development (5P30HD18655). There are no conflicts of interest, and no relationships that would in any way influence or bias this study.
Figures
References
-
- Weindling AM, Wilkinson AR, Cook J, et al. Perinatal events which precede periventricular haemorrhage and leukomalacia in the newborn. Br J Obstet Gynaecol. 1985;92:1218–23. - PubMed
-
- Watkins AM, West CR, Cooke RW. Blood pressure and cerebral haemorrhage and ischaemia in very low birthweight infants. Early Hum Dev. 1989;19:103–10. - PubMed
