

Insulin resistance in obese children and adolescents: HOMA-IR cut-off levels in the prepubertal and pubertal periods
- PMID: 21274322
- PMCID: PMC3005684
- DOI: 10.4274/jcrpe.v2i3.100
Insulin resistance in obese children and adolescents: HOMA-IR cut-off levels in the prepubertal and pubertal periods
Abstract
Objective: Childhood obesity is associated with an increased risk for insulin resistance. The underlying mechanism for the physiological increase in insulin levels in puberty is not clearly understood. The aim of the present study was to determine the cut-off values for homeostasis model assessment for insulin resistance (HOMA-IR) in obese children and adolescents according to gender and pubertal status.
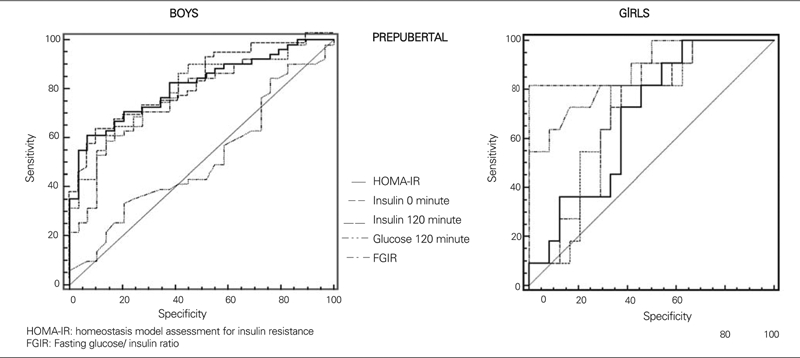
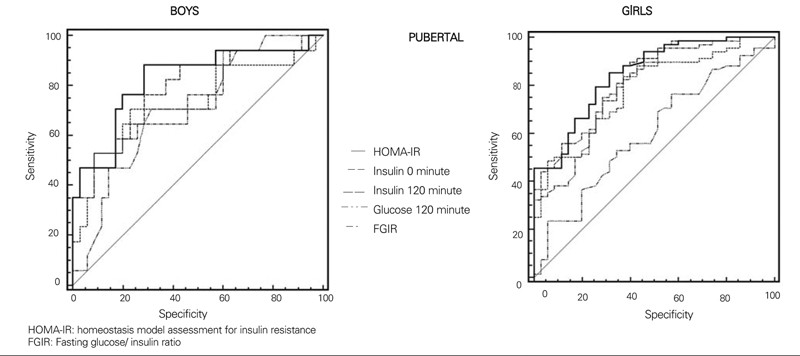
Methods: Two hundred and eight obese children and adolescents (141 girls, 127 boys) aged between 5 and 18 years were included in the study. The children were divided into prepubertal and pubertal groups. A standard oral glucose tolerance test (OGTT) was carried out in all children. A total insulin level exceeding 300 μU/mL in the blood samples, collected during the test period, was taken as the insulin resistance criterion. Cut-off values for HOMA-IR were calculated by receiver operating characteristic (ROC) analysis.
Results: In the prepubertal period, the rate of insulin resistance was found to be 37% in boys and 27.8% in girls,while in the pubertal period, this rate was 61.7% in boys and 66.7% in girls. HOMA-IR cut-off values for insulin resistance in the prepubertal period were calculated to be 2.67 (sensitivity 88.2%, specificity 65.5%) in boys and 2.22 (sensitivity 100%, specificity 42.3%) in girls, and in the pubertal period, they were 5.22 (sensitivity 56%, specificity 93.3%) in boys and 3.82 (sensitivity 77.1%, specificity 71.4%) in girls.
Conclusions: Since gender, obesity and pubertal status are factors affecting insulin resistance, cut-off values which depend on gender and pubertal status, should be used in evaluation of insulin resistance.
Keywords: HOMA−IR cut−off values; gender; insulin resistance; obesity; pubertal status.
Figures
References
-
- Invitti C, Guzzaloni G, Gilardini L, Morabito F, Viberti G. Prevalence and concomitants of glucose intolerance in European obese children and adolescents. Diabetes Care. 2003;26:118–124. - PubMed
-
- Ferrannini E, Buzzigoli G, Bonadonna R, Giorico MA, Oleggini M, Graziadei L, Pedrinelli R, Brandi L, Bevilacqua S. Insulin resistance in essential hypertension. N Engl J Med. 1987;317:350–357. - PubMed
-
- Martin BC, Warram JH, Krolewski AS, Bergman RN, Soeldner JS, Kahn CR. Role of glucose and insulin resistance in development of type 2 diabetes mellitus: results of a 25−year follow−up study. Lancet. 1992;340:925–929. - PubMed
-
- Kahn SE, Prigeon RL, McCulloch DK, Boyko EJ, Bergman RN, Schwartz MW, Neifing JL, Ward WK, Beard JC, Palmer JP. Quantification of the relationship between insulin sensitivity and beta−cell function in human subjects. Evidence for a hyperbolic function. Diabetes. 1993;42:1663–1672. - PubMed
-
- Ten S, Maclaren N. Insulin resistance syndrome in children. J Clin Endocrinol Metab. 2004;89:2526–2539. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical