

Development and reliability testing of the frequency, etiology, direction, and severity (FEDS) system for classifying glenohumeral instability
- PMID: 21277809
- PMCID: PMC3095756
- DOI: 10.1016/j.jse.2010.10.027
Development and reliability testing of the frequency, etiology, direction, and severity (FEDS) system for classifying glenohumeral instability
Abstract
Hypothesis: Classification systems for glenohumeral instability (GHI) are opinion based, not validated, and poorly defined. The hypothesis driving this investigation is that a classification system with content validity will have high inter-observer and intra-observer agreement.
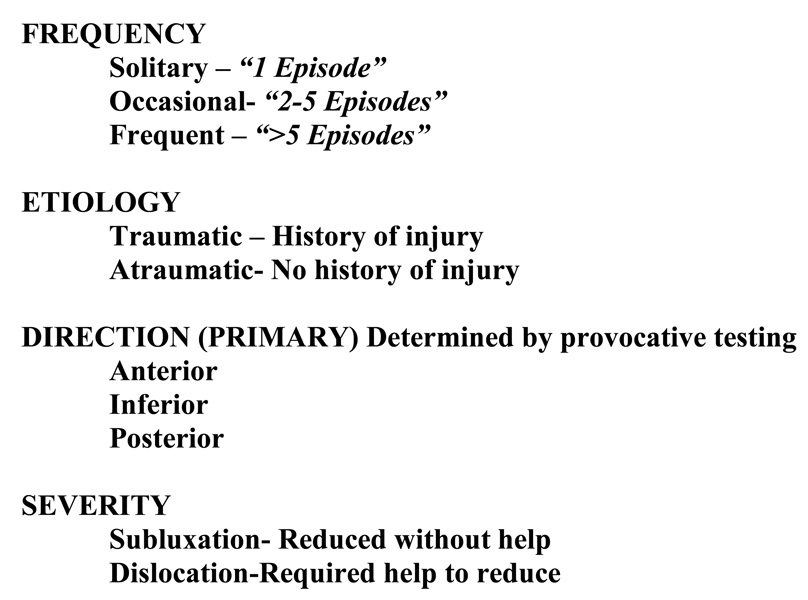
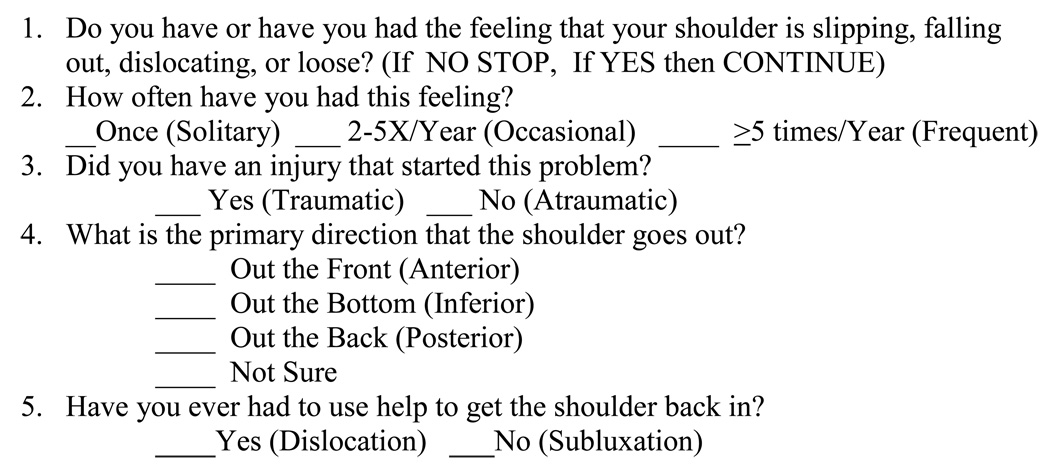
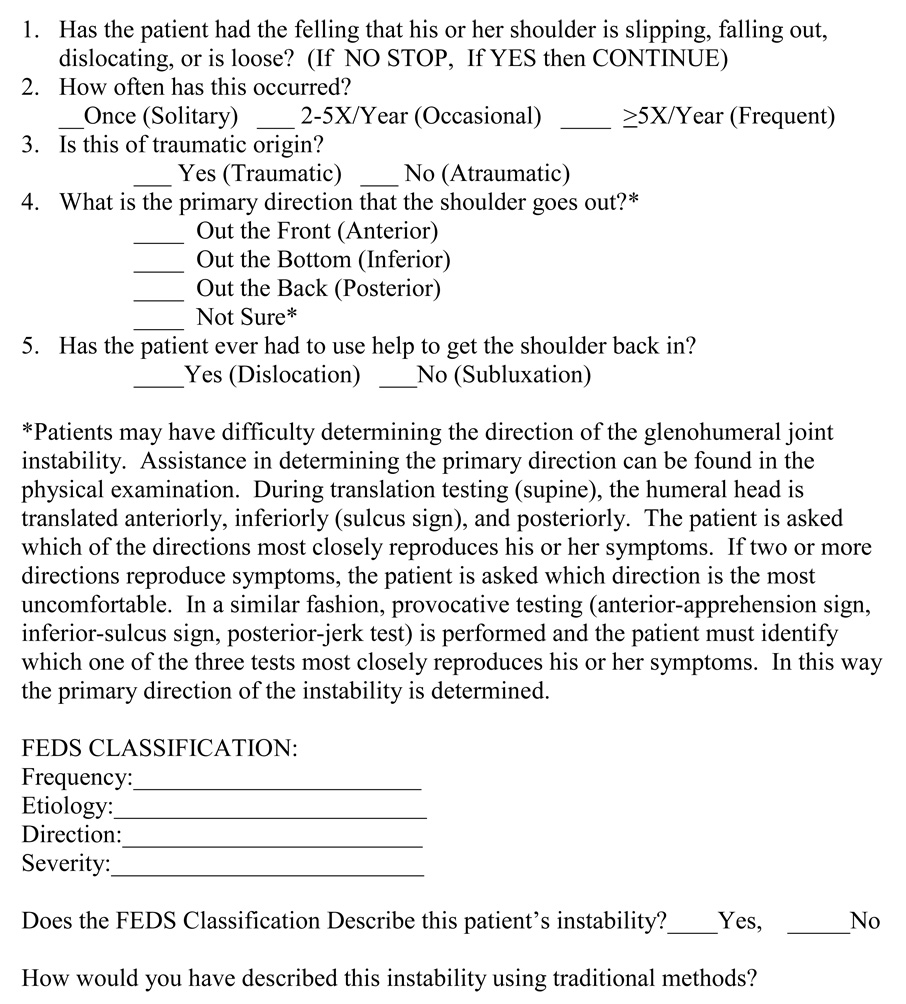
Materials and methods: The classification system was developed by first conducting systematic literature review that identified 18 systems for classifying GHI. The frequency of characteristics used was recorded. Additionally, 31 members of the American Shoulder and Elbow Surgeons responded to a survey to identify features important to characterize GHI. Frequency, etiology, direction, and severity (FEDS) were most important. Frequency was defined as solitary (1 episode), occasional (2 to 5 times/y), or frequent (>5 times/year). Etiology was defined as traumatic or atraumatic. Direction referred to the primary direction of instability (anterior, posterior, or inferior). Severity was subluxation or dislocation. For reliability testing, 50 GHI patients completed a questionnaire at their initial visit. One of 6 sports medicine fellowship-trained physicians completed a similar questionnaire after examining the patient. Patients returned after 2 weeks and were examined by the original physician and 2 other physicians. Interrater and intrarater agreement for the FEDS classification system was calculated.
Results: Agreement between patients and physicians was lowest for frequency (39%; κ = 0.130) and highest for direction (82%; κ = 0.636). Physician intrarater agreement was 84% to 97% for the individual FEDS characteristics (κ = 0.69-0.87), and interrater agreement was 82% to 90% (κ = 0.44-0.76).
Conclusions: The FEDS system has content validity and is highly reliable for classifying GHI. Physical examination using provocative testing to determine the primary direction of instability produces very high levels of interrater and intrarater agreement.
Copyright © 2011 Journal of Shoulder and Elbow Surgery Board of Trustees. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Allen AA. Clinical Evaluation of the Unstable Shoulder. In: Warren RE, Craig EV, Altchek DW, editors. The Unstable Shoulder. Philadelphia: Lippincott-Raven; 1999. pp. 93–106. ISBN-10: 0397516770, ISBN-13: 978-0397516773.
-
- Bahk M, Keyurapan E, Tasaki A, Sauers EL, McFarland EG. Laxity testing of the shoulder: a review. Am J Sports Med. 2007;35(1):131–122. doi:10.1177/0363546506294570 PMid:17130247. - DOI - PubMed
-
- Chahal J, Kassiri K, Dio A, MacDonald P, Leiter J. Diagnostic and treatment differences among experienced shoulder surgeons for instability conditions of the shoulder. Clin J Sport Med. 2007;17:5–9. doi:10.1097/JSM.0b013e31802b4fda. - DOI - PubMed
-
- Cofield RH, Irving JF. Evaluation and classification of shoulder instability. With special reference to examination under anesthesia. Clin Orthop Rel Res. 1987;223:32–43. PMid:3308270. - PubMed
-
- Cole BJ, Warner JJP. Anatomy, Biomechanics, and Pathophysiology of Glenohumeral Instability. In: Iannotti JP, Williams GR, editors. Disorders of the Shoulder. Philadelphia: Lippincott, Williams and Wilkins; 1999. pp. 207–232. ISBN-10: 0781756782, ISBN-13:978-0781756785.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
