

Charcot-Marie-Tooth disease subtypes and genetic testing strategies
- PMID: 21280073
- PMCID: PMC3058597
- DOI: 10.1002/ana.22166
Charcot-Marie-Tooth disease subtypes and genetic testing strategies
Abstract
Objective: Charcot-Marie-Tooth disease (CMT) affects 1 in 2,500 people and is caused by mutations in more than 30 genes. Identifying the genetic cause of CMT is often necessary for family planning, natural history studies, and for entry into clinical trials. However genetic testing can be both expensive and confusing to patients and physicians.
Methods: We analyzed data from 1,024 of our patients to determine the percentage and features of each CMT subtype within this clinic population. We identified distinguishing clinical and physiological features of the subtypes that could be used to direct genetic testing for patients with CMT.
Results: Of 1,024 patients evaluated, 787 received CMT diagnoses. A total of 527 patients with CMT (67%) received a genetic subtype, while 260 did not have a mutation identified. The most common CMT subtypes were CMT1A, CMT1X, hereditary neuropathy with liability to pressure palsies (HNPP), CMT1B, and CMT2A. All other subtypes accounted for less than 1% each. Eleven patients had >1 genetically identified subtype of CMT. Patients with genetically identified CMT were separable into specific groups based on age of onset and the degree of slowing of motor nerve conduction velocities.
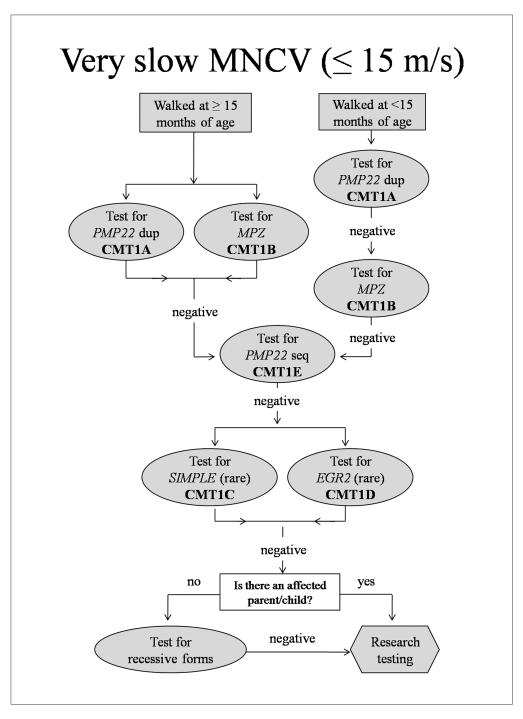
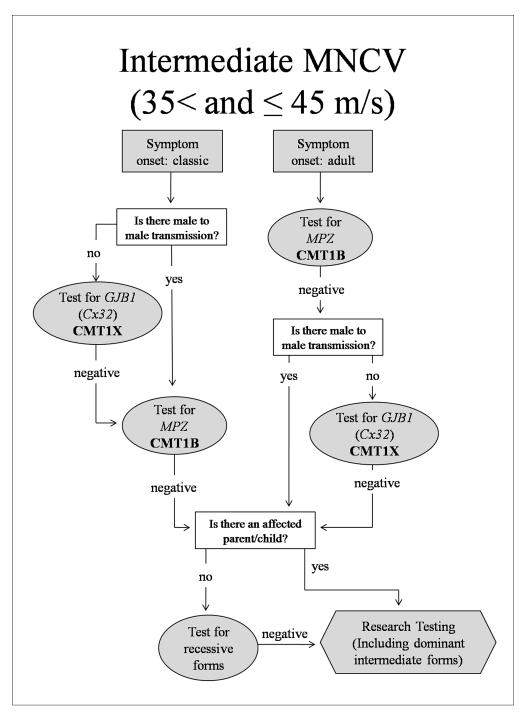
Interpretation: Combining features of the phenotypic and physiology groups allowed us to identify patients who were highly likely to have specific subtypes of CMT. Based on these results, we propose a strategy of focused genetic testing for CMT, illustrated in a series of flow diagrams created as testing guides.
Copyright © 2010 American Neurological Association.
Figures


Comment in
-
The death panel for Charcot-Marie-Tooth panels.Ann Neurol. 2011 Jan;69(1):1-4. doi: 10.1002/ana.22272. Ann Neurol. 2011. PMID: 21280068 No abstract available.
-
Comment: The increasing complexity of phenotype-genotype correlations in CMT.Neurology. 2011 Jul 12;77(2):171. doi: 10.1212/WNL.0b013e3182242dba. Epub 2011 Jun 29. Neurology. 2011. PMID: 21715704 No abstract available.
References
-
- Charcot J, Marie P. Sue une forme particulaire d’atrophie musculaire progressive souvent familial debutant par les pieds et les jamber et atteingnant plus tard les mains. Re Med. 1886;6:97–138.
-
- Tooth H. The peroneal type of progressive muscular atrophy. Lewis; London: 1886.
-
- Skre H. Genetic and clinical aspects of Charcot-Marie-Tooth’s disease. Clin Genet. 1974;6:98–118. - PubMed
-
- Harding AE, Thomas PK. The clinical features of hereditary motor and sensory neuropathy types I and II. Brain. 1980;103:259–280. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
