

Moderate ascites identifies patients with low model for end-stage liver disease scores awaiting liver transplantation who have a high mortality risk
- PMID: 21280185
- PMCID: PMC3058247
- DOI: 10.1002/lt.22218
Moderate ascites identifies patients with low model for end-stage liver disease scores awaiting liver transplantation who have a high mortality risk
Abstract
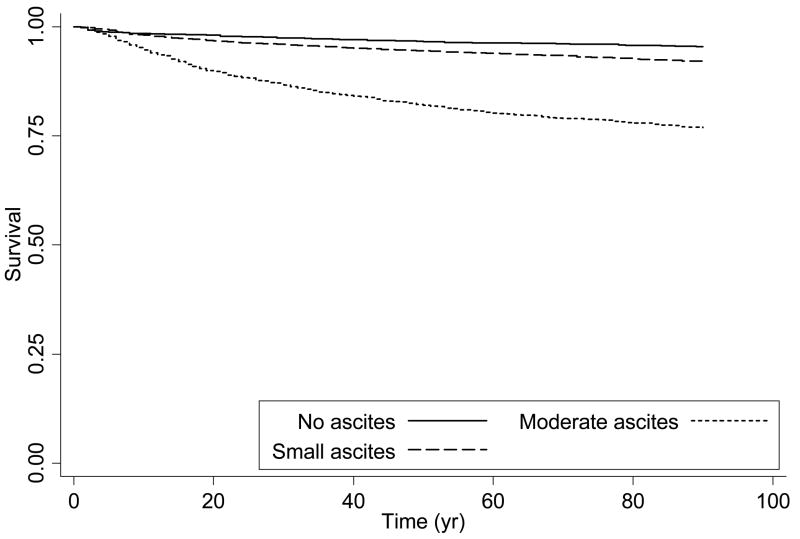
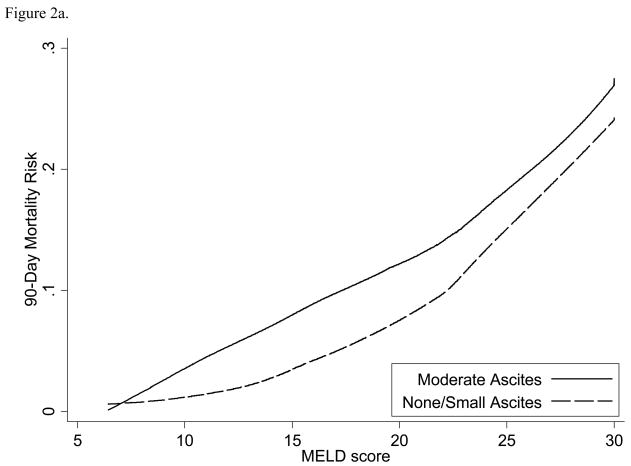
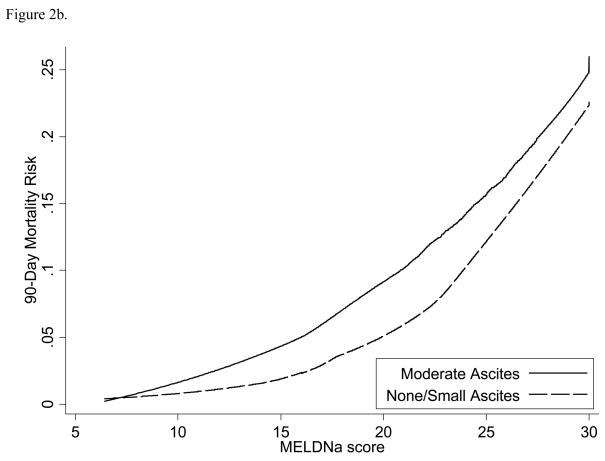
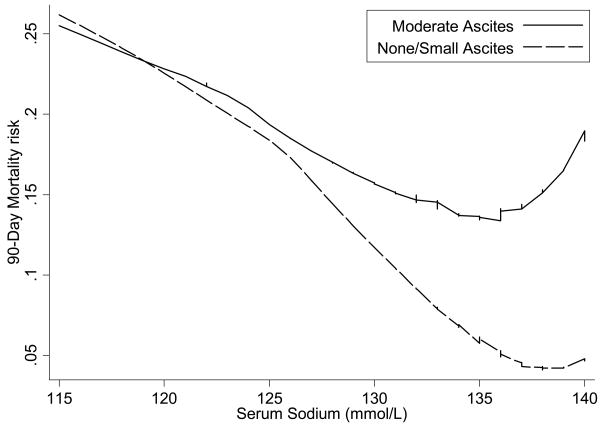
Donor livers are offered to patients with the highest risk of death. How ascites could inform risk models to reduce liver transplant wait-list mortality is unclear. All adult candidates for primary liver transplantation for cirrhosis without exception points who were registered with the Organ Procurement and Transplantation Network from 2005 to 2007 composed our study cohort. Using Cox models and advanced discriminative metrics and paying attention to geographic disparities, we evaluated the additional risk discrimination of moderate ascites over that of the Model for End-Stage Liver Disease (MELD) or the Model for End-Stage Liver Disease plus serum sodium (MELD-Na) alone for the prediction of 90-day wait-list mortality. Additional analyses examined lower mortality risk candidates and those listed in high-demand, low-supply United Network for Organ Sharing regions in which accounting for ascites may most significantly affect wait-list mortality. Between 2005 and 2007, 18,124 subjects were listed for liver transplantation. Mortality was higher in patients with moderate ascites (15.4% versus 6.0%, P < 0.0001), and this risk persisted despite adjustments for MELD (hazard ratio = 1.58, 95% confidence interval = 1.42-1.76) and MELD-Na (hazard ratio = 1.42, 95% confidence interval = 1.28-1.58). The effect of moderate ascites was more prominent with a MELD score <21 (equal to 4.7 MELD units) or with a MELD-Na score <21 (equal to 3.5 MELD-Na units). Wait-list mortality was higher in patients with moderate ascites who were listed in high-demand, limited-supply regions (25.8% versus 17.5% at 1 year, P < 0.01). With the addition of moderate ascites, there was improvement in the overall risk model, particularly with a MELD score <21, as measured by the C index and integrated discrimination improvement. Moderate ascites informed risk prediction, particularly with a MELD score <21 and in high-demand, limited-supply regions. Under the MELD system, the presence of moderate ascites should prompt clinicians to consider strategies to expand access to transplantation, such as the use of extended donor liver grafts.
Copyright © 2011 American Association for the Study of Liver Diseases.
Conflict of interest statement
Figures
Comment in
-
How much is too much?Liver Transpl. 2011 Feb;17(2):102-3. doi: 10.1002/lt.22241. Liver Transpl. 2011. PMID: 21280181 No abstract available.
References
-
- D’Amico G, Morabito A, Pagliaro L, Marubini E. Survival and prognostic indicators in compensated and decompensated cirrhosis. Dig Dis Sci. 1986;31(5):468–475. - PubMed
-
- Child CG, Turcotte JG. Surgery and portal hypertension. Major Probl Clin Surg. 1964;1:1–85. - PubMed
-
- Pugh RN, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. Transection of the oesophagus for bleeding oesophageal varices. Br J Surg. 1973;60(8):646–649. - PubMed
-
- Kamath PS, Wiesner RH, Malinchoc M, Kremers W, Therneau TM, Kosberg CL, et al. A model to predict survival in patients with end-stage liver disease. Hepatology. 2001;33(2):464–470. - PubMed
-
- Wiesner R, Edwards E, Freeman R, Harper A, Kim R, Kamath P, et al. Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterology. 2003;124(1):91–96. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical