

An evaluation of access to health care services along the rural-urban continuum in Canada
- PMID: 21281470
- PMCID: PMC3045284
- DOI: 10.1186/1472-6963-11-20
An evaluation of access to health care services along the rural-urban continuum in Canada
Abstract
Background: Studies comparing the access to health care of rural and urban populations have been contradictory and inconclusive. These studies are complicated by the influence of other factor which have been shown to be related to access and utilization. This study assesses the equity of access to health care services across the rural-urban continuum in Canada before and after taking other determinants of access into account.
Methods: This is a cross-sectional study of the population of the 10 provinces of Canada using data from the Canadian Community Health Survey (CCHS 2.1). Five different measures of access and utilization are compared across the continuum of rural-urban. Known determinants of utilization are taken into account according to Andersen's Health Behaviour Model (HBM); location of residence at the levels of province, health region, and community is also controlled for.
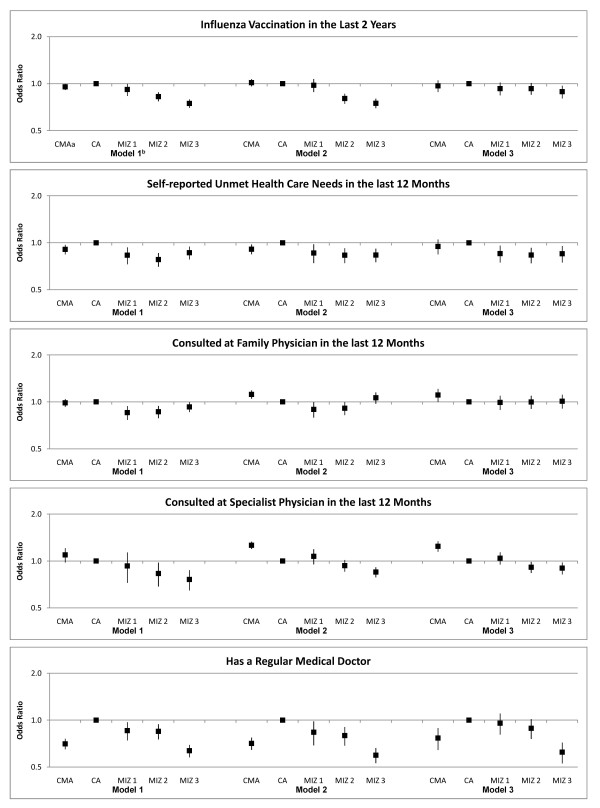
Results: This study found that residents of small cities not adjacent to major centres, had the highest reported utilisation rates of influenza vaccines and family physician services, were most likely to have a regular medical doctor, and were most likely to report unmet need. Among the rural categories there was a gradient with the most rural being least likely to have had a flu shot, use specialist physicians services, or have a regular medical doctor. Residents of the most urban centres were more likely to report using specialist physician services. Many of these differences are diminished or eliminated once other factors are accounted for. After adjusting for other factors those living in the most urban areas were more likely to have seen a specialist physician. Those in rural communities had a lower odds of receiving a flu shot and having a regular medical doctor. People residing in the most urban and most rural communities were less likely to have a regular medical doctor. Those in any of the rural categories were less likely to report unmet need.
Conclusion: Inequities in access to care along the rural-urban continuum exist and can be masked when evaluation is done at a very large scale with gross indicators of rural-urban. Understanding the relationship between rural-urban and other determinants will help policy makers to target interventions appropriately: to specific demographic, provincial, community, or rural categories.
Figures
References
-
- Canada Health Act. http://laws.justice.gc.ca/eng/C-6/index.html
-
- Marchildon GP. The Chaoulli Case: a two-tier Magna Carta? Healthc Q. 2005;8:49–52. 2. - PubMed
-
- Andersen RM, Rice TH, Kominski GF. Changing the U.S. health care systemkey issues in health services, policy, and management. San Francisco: Jossey-Bass; 2001.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
