

Natural antibodies against several pneumococcal virulence proteins in children during the pre-pneumococcal-vaccine era: the generation R study
- PMID: 21282409
- PMCID: PMC3067559
- DOI: 10.1128/IAI.01379-10
Natural antibodies against several pneumococcal virulence proteins in children during the pre-pneumococcal-vaccine era: the generation R study
Abstract
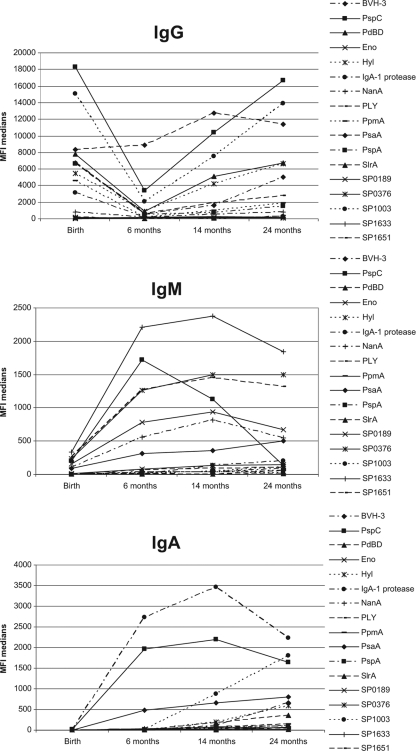
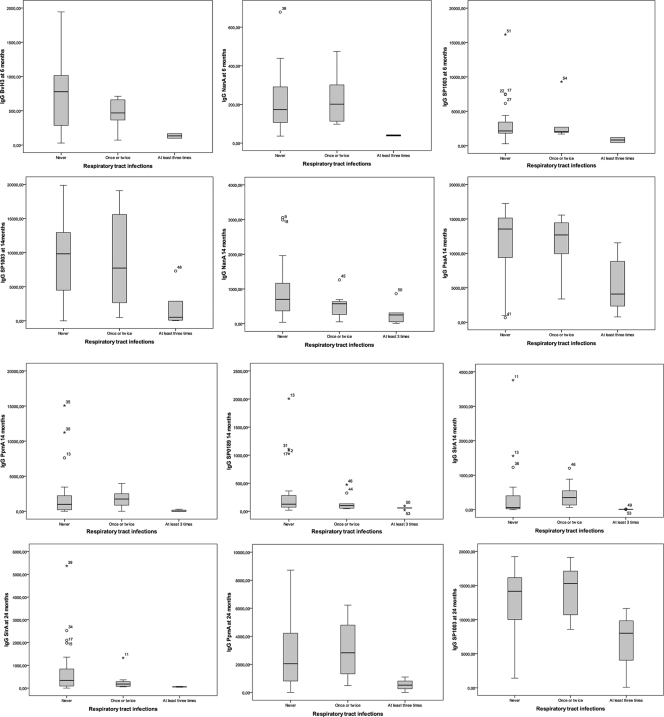
The currently available pneumococcal vaccines do not protect against all serotypes of Streptococcus pneumoniae. A shift toward nonvaccine serotypes causing colonization and invasive disease has occurred, and studies on protein-based vaccines have been undertaken. We assessed the association between specific antibodies against pneumococcal virulence proteins and colonization and respiratory tract infections (RTIs). Additionally, we assessed the extent to which colonization induces a humoral immune response. Nasopharyngeal swabs collected from children at 1.5, 6, 14, and 24 months of age were cultured for pneumococcus. Serum samples were obtained at birth and at 6, 14, and 24 months (n = 57 children providing 177 serum samples). Data were collected prior to the pneumococcal vaccine era. IgG, IgA, and IgM levels against 17 pneumococcal protein vaccine candidates were measured using a bead-based flow cytometry technique (xMAP; Luminex Corporation). Information regarding RTIs was questionnaire derived. Levels of IgG against all proteins were high in cord blood, decreased in the first 6 months and increased again thereafter, in contrast to the course of IgA and IgM levels. Specific antibodies were induced upon colonization. Increased levels of IgG against BVH-3, NanA, and SP1003 at 6 months, NanA, PpmA, PsaA, SlrA, SP0189, and SP1003 at 14 months, and SlrA at 24 months were associated with a decreased number of RTIs in the third year of life but not with colonization. Maternal antipneumococcal antibodies did not protect against pneumococcal colonization and infection. Certain antibodies against pneumococcal virulence proteins, some of which are induced by colonization, are associated with a decreased number of RTIs in children. This should be taken into account in future pneumococcal vaccine studies.
Figures
References
-
- Adrian, P. V., et al. 2004. Development of antibodies against pneumococcal proteins alpha-enolase, immunoglobulin A1 protease, streptococcal lipoprotein rotamase A, and putative proteinase maturation protein A in relation to pneumococcal carriage and otitis media. Vaccine 22:2737-2742. - PubMed
-
- Bogaert, D., R. De Groot, and P. W. Hermans. 2004. Streptococcus pneumoniae colonisation: the key to pneumococcal disease. Lancet Infect. Dis. 4:144-154. - PubMed
-
- Bogaert, D., P. W. Hermans, P. V. Adrian, H. C. Rumke, and R. de Groot. 2004. Pneumococcal vaccines: an update on current strategies. Vaccine 22:2209-2220. - PubMed
-
- Bogaert, D., et al. 2006. Development of antibodies against the putative proteinase maturation protein A in relation to pneumococcal carriage and otitis media. FEMS Immunol. Med. Microbiol. 46:166-168. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
