

Atazanavir pharmacokinetics with and without tenofovir during pregnancy
- PMID: 21283017
- PMCID: PMC3125419
- DOI: 10.1097/QAI.0b013e31820fd093
Atazanavir pharmacokinetics with and without tenofovir during pregnancy
Abstract
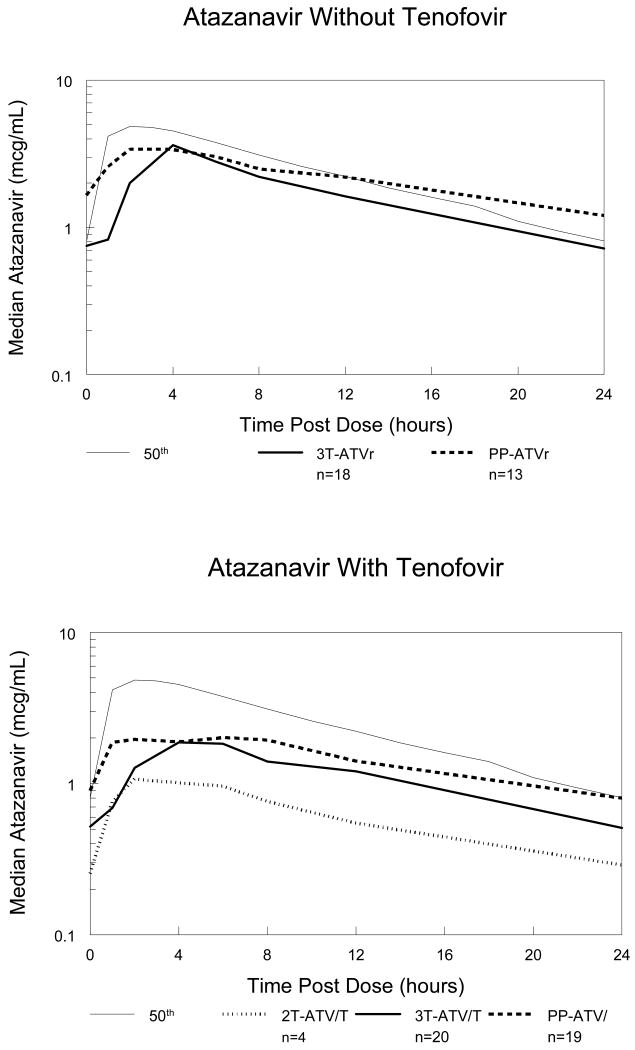
Background: Few data are available describing atazanavir exposure during pregnancy, especially when used in combination with tenofovir, whose coadministration with atazanavir results in decreased atazanavir exposure.
Design: International Maternal Pediatric Adolescent AIDS Clinical Trials 1026 s is an ongoing, prospective, nonblinded study of antiretroviral pharmacokinetics in HIV-infected pregnant women that included 2 cohorts receiving atazanavir/ritonavir 300 mg/100 mg once daily, either with or without tenofovir.
Methods: Intensive steady-state 24-hour pharmacokinetic profiles were performed during the third trimester and at 6-12 weeks postpartum. Atazanavir was measured by reverse-phase high-performance liquid chromatography (detection limit 0.047 mcg/mL). Pharmacokinetic targets were the estimated 10th percentile atazanavir area under the concentration versus time curve [(AUC): 29.4 mcg · hr · mL-1] in nonpregnant historical controls (mean AUC = 57 mcg · hr · mL-1) and a trough concentration of 0.15 mcg/mL, the concentration target used in therapeutic drug monitoring programs.
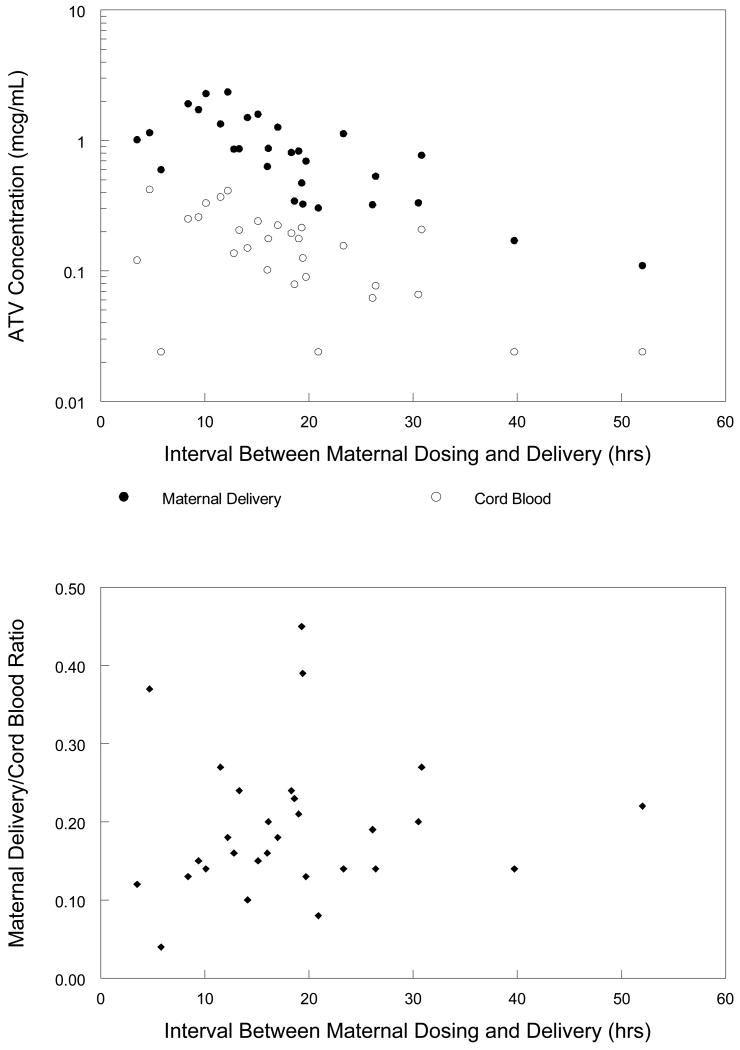
Results: Median atazanavir AUC was reduced during the third trimester compared with postpartum for subjects not receiving tenofovir (41.9 vs. 57.9 mcg · hr · mL-1, P = 0.02) and for subjects receiving tenofovir (28.8 vs. 39.6 mcg · hr · mL-1, P = 0.04). During the third trimester, AUC was below the target in 33% (6 of 18) of women not receiving tenofovir and 55% (11 of 20) of women receiving tenofovir. Trough concentration was below the target in 6% (1 of 18) of women not receiving tenofovir and 15% (3 of 20) of women receiving tenofovir. The median (range) ratio of cord blood/maternal atazanavir concentration in 29-paired samples was 0.18 (0-0.45).
Conclusions: Atazanavir exposure is reduced by pregnancy and by concomitant tenofovir use. A dose increase of atazanavir/ritonavir to 400 mg/100 mg may be necessary in pregnant women to ensure atazanavir exposure equivalent to that seen in nonpregnant adults.
Figures
References
-
- Shapiro D, T R, Pollack H, et al. Mother-to-child HIV transmission risk according to antiretroviral therapy, mode of delivery and viral load in 2895 US women (PACTG 367). Paper presented at: Program and Abstracts of the 11th Conference on Retroviruses and Opportunistic Infections; Feb. 2004; San Francisco, CA. Abstract 99.
-
- Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-1-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV Transmission in the United States. May 242010. [May 24, 2010]. pp. 1–117. Available at http://aidsinfo.nih.gov/ContentFiles/PerinatalGL.pdf.
-
- Stek AM, Mirochnick M, Capparelli E, et al. Reduced lopinavir exposure during pregnancy. AIDS. 2006 Oct 3;20(15):1931–1939. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
