

The case for reactive mass oral cholera vaccinations
- PMID: 21283614
- PMCID: PMC3026767
- DOI: 10.1371/journal.pntd.0000952
The case for reactive mass oral cholera vaccinations
Abstract
Introduction: The outbreak of cholera in Zimbabwe intensified interest in the control and prevention of cholera. While there is agreement that safe water, sanitation, and personal hygiene are ideal for the long term control of cholera, there is controversy about the role of newer approaches such as oral cholera vaccines (OCVs). In October 2009 the Strategic Advisory Group of Experts advised the World Health Organization to consider reactive vaccination campaigns in response to large cholera outbreaks. To evaluate the potential benefit of this pivotal change in WHO policy, we used existing data from cholera outbreaks to simulate the number of cholera cases preventable by reactive mass vaccination.
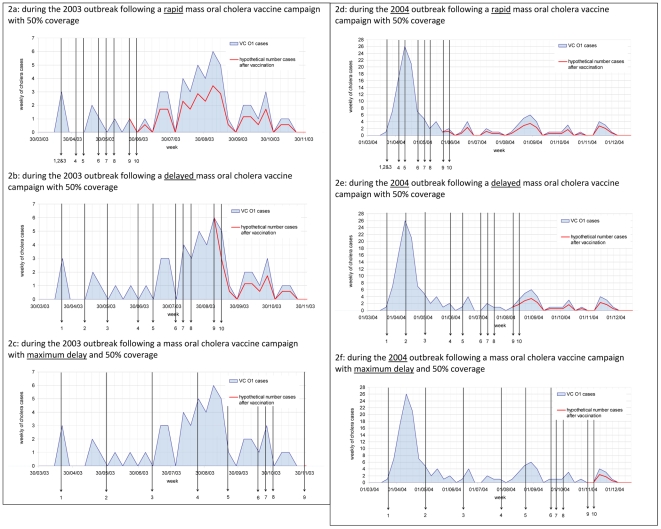
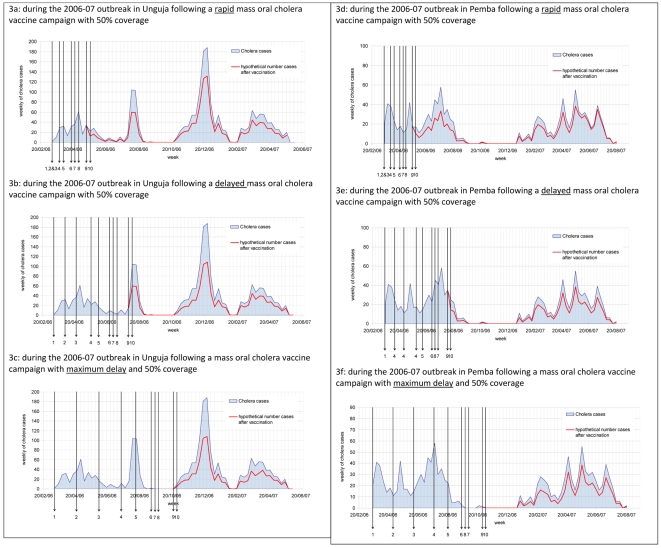
Methods: Datasets of cholera outbreaks from three sites with varying cholera endemicity--Zimbabwe, Kolkata (India), and Zanzibar (Tanzania)--were analysed to estimate the number of cholera cases preventable under differing response times, vaccine coverage, and vaccine doses.
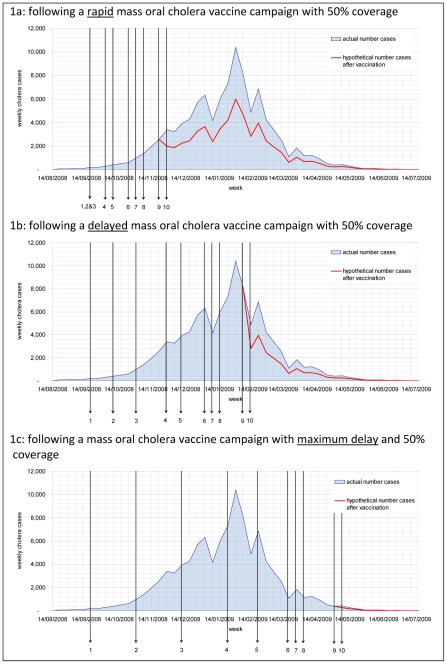
Findings: The large cholera outbreak in Zimbabwe started in mid August 2008 and by July 2009, 98,591 cholera cases had been reported with 4,288 deaths attributed to cholera. If a rapid response had taken place and half of the population had been vaccinated once the first 400 cases had occurred, as many as 34,900 (40%) cholera cases and 1,695 deaths (40%) could have been prevented. In the sites with endemic cholera, Kolkata and Zanzibar, a significant number of cases could have been prevented but the impact would have been less dramatic. A brisk response is required for outbreaks with the majority of cases occurring during the early weeks. Even a delayed response can save a substantial number of cases and deaths in long, drawn-out outbreaks. If circumstances prevent a rapid response there are good reasons to roll out cholera mass vaccination campaigns well into the outbreak. Once a substantial proportion of a population is vaccinated, outbreaks in subsequent years may be reduced if not prevented. A single dose vaccine would be of advantage in short, small outbreaks.
Conclusions: We show that reactive vaccine use can prevent cholera cases and is a rational response to cholera outbreaks in endemic and non-endemic settings. In large and long outbreaks a reactive vaccination with a two-dose vaccine can prevent a substantial proportion of cases. To make mass vaccination campaigns successful, it would be essential to agree when to implement reactive vaccination campaigns and to have a dynamic and determined response team that is familiar with the logistic challenges on standby. Most importantly, the decision makers in donor and recipient countries have to be convinced of the benefit of reactive cholera vaccinations.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- WHO. Meeting of the Strategic Advisory Group of Experts on immunization, October 2009 – conclusions and recommendations. Weekly epidemiological record. 2009;50:526–528. - PubMed
-
- WHO. Outbreak News Cholera, Zimbabwe. Weekly epidemiological record. 2008;83:449–450. - PubMed
-
- Bhattacharya S, Black R, Bourgeois L, Clemens J, Cravioto A, et al. Public health. The cholera crisis in Africa. Science. 2009;324:885. - PubMed
-
- WHO. Outbreak News Cholera, Zimbabwe. Weekly epidemiological record. 2009;84:517–532.
-
- WHO. Cholera, 2008. Weekly epidemiological record. 2009;84:309–324.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
