

Review
doi: 10.1186/1479-5876-9-S1-S5.
Clinical significance of HIV-1 coreceptor usage
Affiliations
- PMID: 21284904
- PMCID: PMC3105505
- DOI: 10.1186/1479-5876-9-S1-S5
Item in Clipboard
Review
Clinical significance of HIV-1 coreceptor usage
J Transl Med.
.
Abstract
The identification of phenotypically distinct HIV-1 variants with different prevalence during the progression of the disease has been one of the earliest discoveries in HIV-1 biology, but its relevance to AIDS pathogenesis remains only partially understood. The physiological basis for the phenotypic variability of HIV-1 was elucidated with the discovery of distinct coreceptors employed by the virus to infect susceptible cells. The role of the viral phenotype in the variable clinical course and treatment outcome of HIV-1 infection has been extensively investigated over the past two decades. In this review, we summarize the major findings on the clinical significance of the HIV-1 coreceptor usage.
Figures

Overview of coreceptor use and cell tropism of different HIV-1 variants. Individual viral isolates are classified based on their ability to use CCR5 (R5 variants), CXCR4 (X4 variants) or both coreceptors (R5X4 variants). Bulk viral isolates capable of using both coreceptors are designated dual/mixed (D/M) as their quasispecies may contain any mixture of the various phenotypic variants. The cell tropism of each viral isolate is determined by the expression levels of CCR5 and CXCR4 on the various target cells.
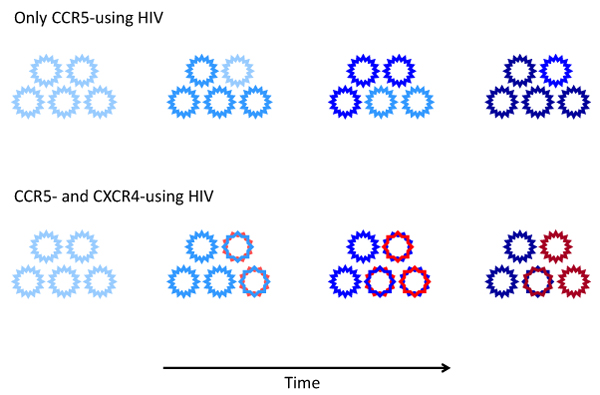
Evolution of HIV-1 coreceptor usage during the progression of the disease. In most individuals HIV-1 infection is initially sustained by CCR5-using variants (R5, blue). In ~50% of the patients infected with subtype-B HIV-1, the CCR5-using variants acquire the ability to use CXCR4 (R5X4, blue/red) prior to AIDS diagnosis. Subsequently, these dual-tropic R5X4 variants may lose their ability to use CCR5 (X4 variants, red). Over time, viral coreceptor usage evolves resulting in viral variants with increased affinity for their respective coreceptor (increased color intensity).

Typical course of HIV-1 disease in relation to HIV-1 coreceptor usage. (A) Individual infected with pure R5 variants: constant rate of CD4 decline and viral load incline. (B) Individual with emergence of CXCR4-using variants in the course of infection: accelerated CD4 decline, viral load incline and disease progression upon emergence of CXCR4-using variants. While CXCR4-using variants can emerge at any stage of infection, untreated individuals who develop such variants progress to AIDS within an average of 2 years after their first detection.

Time between seroconversion (SC) and AIDS among participants in the Amsterdam Cohort Studies on HIV infection and AIDS with or without CXCR4-using variants detected prior to AIDS diagnosis. All homosexual and drug-user participants with AIDS diagnosis according to the 1993 CDC definition prior to initiation of effective antiretroviral therapy were included in the analysis. Participants were divided into 2 groups based on the presence (X4, closed circles) or absence (R5, open circles) of CXCR4-using HIV-1 variants as detected by the MT-2 assay prior to AIDS diagnosis. Time between SC and AIDS was categorized in 12-monthly intervals. The graph shows the proportion of participants per category as a percentage of the total number of participants in the group.
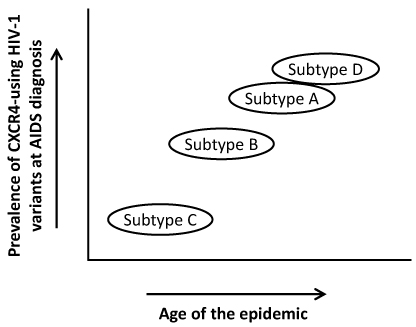
Hypothetical model of the evolutionary dynamics of CXCR4 usage in relation to the age of each HIV-1 subtype epidemic. Recent data suggest that the proportion of patients with detectable emergence of CXCR4-using HIV-1 variants varies in relation to the age of the different subtype epidemics, with subtype D (high CXCR4 switch rate) being the oldest and subtype C (low CXCR4 switch rate) the youngest.
References
-
- Huang W, Eshleman SH, Toma J, Fransen S, Stawiski E, Paxinos EE, Whitcomb JM, Young AM, Donnell D, Mmiro F. et al. Coreceptor tropism in human immunodeficiency virus type 1 subtype D: high prevalence of CXCR4 tropism and heterogeneous composition of viral populations. J Virol. 2007;81:7885–7893. doi: 10.1128/JVI.00218-07. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
