

A multi-centre randomised phase III trial of Dexamethasone vs Dexamethasone and diethylstilbestrol in castration-resistant prostate cancer: immediate vs deferred Diethylstilbestrol
- PMID: 21285990
- PMCID: PMC3049603
- DOI: 10.1038/bjc.2011.7
A multi-centre randomised phase III trial of Dexamethasone vs Dexamethasone and diethylstilbestrol in castration-resistant prostate cancer: immediate vs deferred Diethylstilbestrol
Abstract
Background: The role of further hormone therapy in castration-resistant prostate cancer (CRPC) remains unclear. We performed a multi-centre randomised phase III study comparing the use of Dexamethasone, Aspirin, and immediate addition of Diethylstilbestrol (DAiS) vs Dexamethasone, Aspirin, and deferred (until disease progression) addition of Diethylstilbestrol (DAdS).
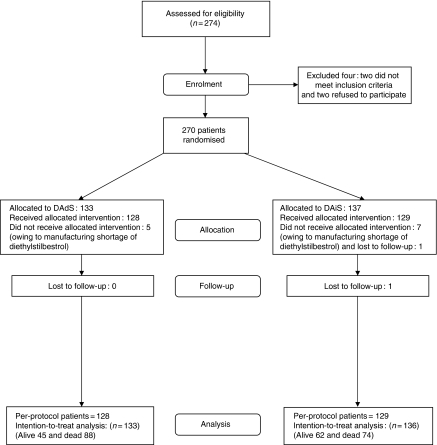
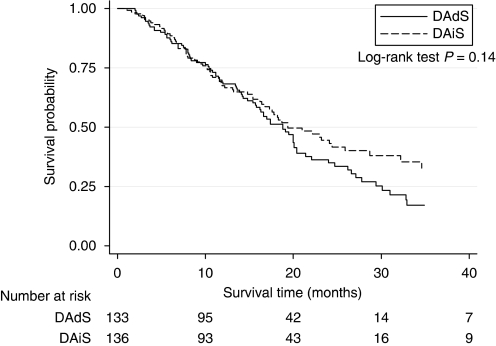
Methods: From 2001 to 2008, 270 men with chemotherapy-naive CRPC were randomly assigned, in a 1 : 1 ratio, to receive either DAiS or DAdS. They were stratified for performance status, presence of bone metastases, and previous normalisation of prostate-specific antigen (PSA) to androgen deprivation. The study end points were the proportion of patients achieving a 50% PSA response, progression-free survival (PFS), overall survival, and quality of life. Intention-to-treat analysis was carried out. The effect of treatment was studied first by Kaplan-Meier curves and log-rank test, and finally through multivariable stratified Cox's proportional hazards model adjusting for the effects of possible baseline prognostic factors. Quality of life was analysed using multivariate analysis of variance.
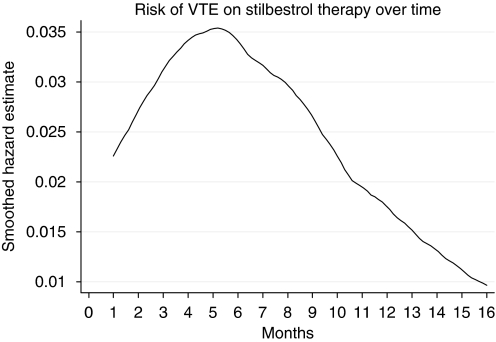
Results: At study entry, the median age was 76 years (inter-quartile range: 70-80 years), the median PSA was 79 ng ml(-1), and 76% of the cohort had metastatic disease. The response rates for DAiS (68%) and DAdS (64%) were not significantly different (P=0.49). Similar to the response rate, neither the PFS (median=8.1 months for both arms) nor the overall survival (19.4 vs 18.8 months) differed significantly between the DAiS and DAdS groups (P>0.20). However, the response rate for the DAiS (68%) was significantly higher than the response rate of DA (before adding Diethylstilbestrol) (50%) (P=0.002). Similarly, the median time to progression for DAiS (8.6 months) was significantly longer than that of DA (4.5 months) (P<0.001). Multivariable analysis showed that patients with previous haemoglobin ≥11 g dl(-1) decreased the risk of death significantly (hazard ratio: 0.44, 95% CI: 0.25-0.77). Patients treated with previous anti-androgens alone had more than 5 times more risk of death compared with patients treated with gonadorelin analogues throughout their castration-sensitive phase. Treatment sequencing did not affect the quality of life but pre-treatment performance status did. The incidence of veno-thromboembolic events was 22% (n=28) in DAiS and 11% (n=14) in the DA arm (P=0.02). Painful gynaecomastia occurred in only 1% on DA, whereas in 40% on DAiS (P=0.001).
Conclusion: Dexamethasone and immediate Diethylstilbestrol resulted in neither higher PSA response rate nor higher PFS compared with Dexamethasone with deferred Diethylstilbestrol. There was no suggestion of significantly improved overall survival or quality of life. Given the significantly higher toxicity of Diethylstilbestrol, deferring Diethylstilbestrol until failure of Dexamethasone is the preferred strategy when using these agents in CRPC.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Attard G, Reid AH, A'Hern R, Parker C, Oommen NB, Folkerd E, Messiou C, Molife LR, Maier G, Thompson E, Olmos D, Sinha R, Lee G, Dowsett M, Kaye SB, Dearnaley D, Kheoh T, Molina A, de Bono JS (2009) Selective inhibition of CYP17 with abiraterone acetate is highly active in the treatment of castration-resistant prostate cancer. J Clin Oncol 27(23): 3742–3748 - PMC - PubMed
-
- Attard G, Reid AH, Yap TA, Raynaud F, Dowsett M, Settatree S, Barrett M, Parker C, Martins V, Folkerd E, Clark J, Cooper CS, Kaye SB, Dearnaley D, Lee G, de Bono JS (2008) Phase I clinical trial of a selective inhibitor of CYP17, abiraterone acetate, confirms that castration-resistant prostate cancer commonly remains hormone driven. J Clin Oncol 26(28): 4563–4571 - PubMed
-
- Bubley GJ, Carducci M, Dahut W, Dawson N, Daliani D, Eisenberger M, Figg WD, Freidlin B, Halabi S, Hudes G, Hussain M, Kaplan R, Myers C, Oh W, Petrylak DP, Reed E, Roth B, Sartor O, Scher H, Simons J, Sinibaldi V, Small EJ, Smith MR, Trump DL, Vollmer R, Wilding G (1999) Eligibility and response guidelines for phase II clinical trials in androgen-independent prostate cancer: recommendations from the Prostate-Specific Antigen Working Group. J Clin Oncol 17(11): 3461–3467 - PubMed
-
- Farrugia D, Ansell W, Singh M, Philp T, Chinegwundoh F, Oliver RT (2000) Stilboestrol plus adrenal suppression as salvage treatment for patients failing treatment with luteinizing hormone-releasing hormone analogues and orchidectomy. BJU Int 85(9): 1069–1073 - PubMed
-
- Fossa SD, Slee TPH, Brausi M, Horenblas S, Hall RR, Hetherington JW, Aaronson N, Prijck L, de Collette L (2001) Flutamide vs Prednisone in patients with prostate cancer symptomatically progressing after androgen ablative therapy – a phase III study of the European Organization for Reseach and Treatment of Cancer Genitourinary Group. J Clin Oncol 19: 62–71 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
