

Peritoneovenous shunt for intractable ascites due to hepatic lymphorrhea after hepatectomy
- PMID: 21286221
- PMCID: PMC3030739
- DOI: 10.4240/wjgs.v3.i1.16
Peritoneovenous shunt for intractable ascites due to hepatic lymphorrhea after hepatectomy
Abstract
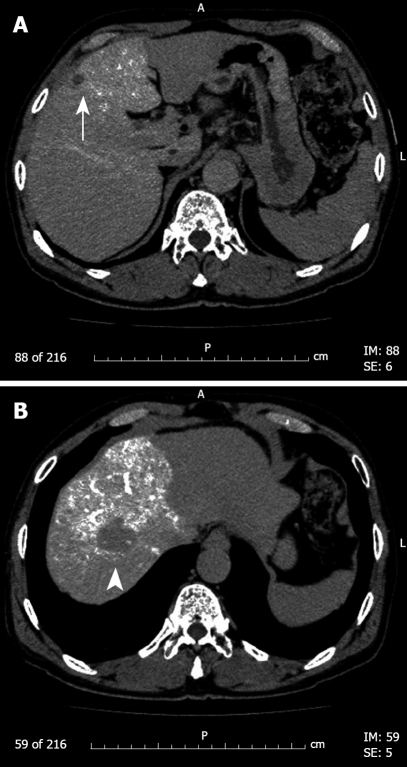
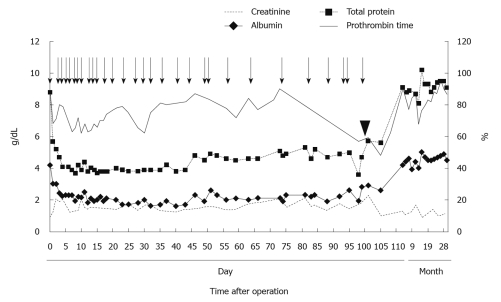
A peritoneovenous shunt has become one of the most efficient procedures for intractable ascites due to liver cirrhosis. A case of intractable ascites due to hepatic lymphorrhea after hepatectomy for hepatocellular carcinoma that was successfully treated by the placement of a peritoneovenous shunt is presented. A 72-year-old Japanese man underwent partial resection of the liver for hepatocellular carcinoma associated with hepatitis C viral infection. After hepatectomy, a considerable amount of ascites ranging from 800-4600 mL per day persisted despite conservative therapy, including numerous infusions of albumin and plasma protein fraction and administration of diuretics. Since the patient's general condition deteriorated, based on the diagnosis of intractable hepatic lymphorrhea, a subcutaneous peritoneovenous shunt was inserted. The patient's postoperative course was uneventful and the ascites decreased rapidly, with serum total protein and albumin levels and hepatic function improving accordingly. For intractable ascites due to hepatic lymphorrhea after hepatectomy, we recommend the placement of a peritoneovenous shunt as a procedure that can provide immediate effectiveness without increased surgical risk.
Keywords: Hepatic lymphorrhea; Hepatocellular carcinoma; Intractable ascites; Peritoneovenous shunt; Surgical procedure.
Figures
References
-
- Ota H, Miyazawa T, Hiizu I, Ueda N, Maeura Y, Matsunaga S, Tomita K. A case report of intractable ascites due to hepatic lymphorrhea from hepatoduodenal ligament after radical gastrectomy for gastric cancer (In Japanese with English abstract) Jpn J Gastroenterol Surg. 1993;26:1115–1119.
-
- Kawahira Y, Nakao K, Nakahara M, Hamaji M, Ogino N, Miyazaki S. A case of intractable hepatic lymphorrhea after gastrectomy for gastric cancer (In Japanese with English abstract) Jpn J Gastroenterol Surg. 1994;27:117–120.
-
- Endo M, Maruyama K, Kinoshita T, Sasako M. Chylous ascites after extended lymphnode dissection for gastric cancer (In Japanese with English abstract) Jpn J Gastroenterol Surg. 1994;27:917–921.
-
- Tanaka K, Ohmori Y, Mohri Y, Tonouchi H, Suematsu M, Taguchi Y, Adachi Y, Kusunoki M. Successful treatment of refractory hepatic lymphorrhea after gastrectomy for early gastric cancer, using surgical ligation and subsequent OK-432 (Picibanil) sclerotherapy. Gastric Cancer. 2004;7:117–121. - PubMed
-
- Miyamoto K, Kusumoto C, Kawabata Y. The effectiveness of Denver peritoneovenous shunt for the treatment of refractory ascites (In Japanese with English abstract) Jpn J Gastroenterol Surg. 2006;39:422–427.
LinkOut - more resources
Full Text Sources
