

Rebleeding rates following TIPS for variceal hemorrhage in the Viatorr era: TIPS alone versus TIPS with variceal embolization
- PMID: 21286346
- PMCID: PMC2994622
- DOI: 10.1007/s12072-010-9206-2
Rebleeding rates following TIPS for variceal hemorrhage in the Viatorr era: TIPS alone versus TIPS with variceal embolization
Abstract
Purpose: To compare rebleeding rates following treatment of variceal hemorrhage with TIPS alone versus TIPS with variceal embolization in the covered stent-graft era.
Methods: In this retrospective study, 52 patients (M:F 29:23, median age 52 years) with hepatic cirrhosis and variceal hemorrhage underwent TIPS insertion between 2003 and 2008. Median Child-Pugh and MELD scores were 8.5 and 13.5. Generally, 10-mm diameter TIPS were created using covered stent-grafts (Viatorr; W.L. Gore and Associates, Flagstaff, AZ). A total of 37 patients underwent TIPS alone, while 15 patients underwent TIPS with variceal embolization. The rates of rebleeding and survival were compared.
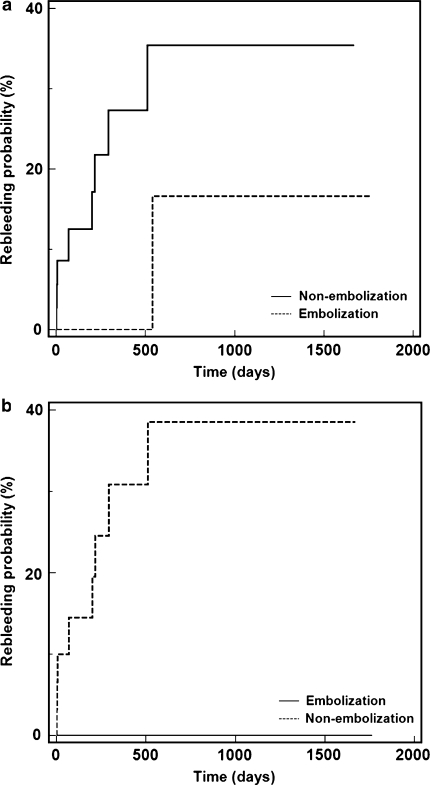
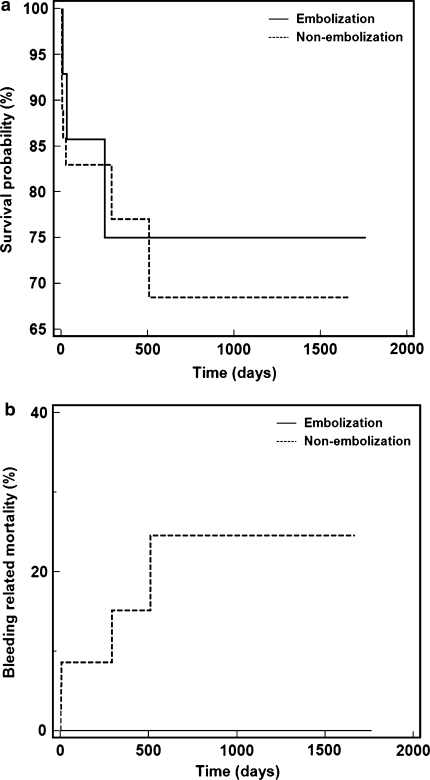
Results: All TIPS were technically successful. Median portosystemic pressure gradient reductions were 13 versus 11 mmHg in the embolization and non-embolization groups. There were no statistically significant differences in Child-Pugh and MELD score, or portosystemic pressure gradients between each group. A trend toward increased rebleeding was present in the non-embolization group, where 8/37 (21.6%) patients rebled while 1/15 (6.7%) patients in the TIPS with embolization group rebled (P = 0.159) during median follow-up periods of 199 and 252 days (P = 0.374). Rebleeding approached statistical significance among patients with acute hemorrhage, where 8/32 (25%) versus 0/14 (0%) rebled in the non-embolization and embolization groups (P = 0.055). A trend toward increased bleeding-related mortality was seen in the non-embolization group (P = 0.120).
Conclusions: TIPS alone showed a high incidence of rebleeding in this series, whereas TIPS with variceal embolization resulted in reduced recurrent hemorrhage. The efficacy of embolization during TIPS performed for variceal hemorrhage versus TIPS alone should be further compared with larger prospective randomized trials.
Keywords: Embolization; Rebleeding; Transjugular intrahepatic portosystemic shunt (TIPS); Variceal hemorrhage.
Figures
Similar articles
-
TIPS for treatment of variceal hemorrhage: clinical outcomes in 128 patients at a single institution over a 12-year period.J Vasc Interv Radiol. 2012 Feb;23(2):227-35. doi: 10.1016/j.jvir.2011.10.015. Epub 2011 Dec 16. J Vasc Interv Radiol. 2012. PMID: 22178037
-
Controlled underdilation using novel VIATORR® controlled expansion stents improves survival after transjugular intrahepatic portosystemic shunt implantation.JHEP Rep. 2021 Mar 3;3(3):100264. doi: 10.1016/j.jhepr.2021.100264. eCollection 2021 Jun. JHEP Rep. 2021. PMID: 34013182 Free PMC article.
-
Adjuvant Transjugular Variceal Occlusion at Creation of a Transjugular Intrahepatic Portosystemic Shunt (TIPS): Efficacy and Risks of Bucrylate Embolization.Cardiovasc Intervent Radiol. 2019 May;42(5):729-736. doi: 10.1007/s00270-019-02176-y. Epub 2019 Feb 20. Cardiovasc Intervent Radiol. 2019. PMID: 30788517
-
Early transjugular intrahepatic portosystemic shunt for acute variceal bleeding: a systematic review and meta-analysis.Eur Radiol. 2021 Jul;31(7):5390-5399. doi: 10.1007/s00330-020-07525-x. Epub 2021 Jan 6. Eur Radiol. 2021. PMID: 33409783
-
Transjugular Intrahepatic Portosystemic Shunt (TIPS): Pathophysiologic Basics, Actual Indications and Results with Review of the Literature.Rofo. 2018 Aug;190(8):701-711. doi: 10.1055/a-0628-7347. Epub 2018 Jul 25. Rofo. 2018. PMID: 30045395 Review. English, German.
Cited by
-
Transjugular intrahepatic portosystemic shunts and portal hypertension-related complications.World J Gastroenterol. 2014 Dec 7;20(45):16996-7010. doi: 10.3748/wjg.v20.i45.16996. World J Gastroenterol. 2014. PMID: 25493012 Free PMC article. Review.
-
Transjugular Intrahepatic Portosystemic Shunt With or Without Gastroesophageal Variceal Embolization for the Prevention of Variceal Rebleeding: A Systematic Review and Meta-Analysis.Gastroenterology Res. 2023 Apr;16(2):68-78. doi: 10.14740/gr1618. Epub 2023 Apr 28. Gastroenterology Res. 2023. PMID: 37187555 Free PMC article.
-
Comparison of embolic agents for varices during transjugular intrahepatic portosystemic shunt for variceal bleeding: Tissue gel or coil?J Interv Med. 2020 Aug 17;3(4):195-200. doi: 10.1016/j.jimed.2020.08.008. eCollection 2020 Dec. J Interv Med. 2020. PMID: 34805934 Free PMC article.
-
Historical overview and review of current day treatment in the management of acute variceal haemorrhage.World J Gastroenterol. 2014 Jun 7;20(21):6481-94. doi: 10.3748/wjg.v20.i21.6481. World J Gastroenterol. 2014. PMID: 24914369 Free PMC article. Review.
-
Comparative outcome of transjugular intrahepatic portosystemic shunt with or without variceal obliteration: a systematic review and meta-analysis.Abdom Radiol (NY). 2023 Apr;48(4):1429-1437. doi: 10.1007/s00261-023-03843-y. Epub 2023 Feb 23. Abdom Radiol (NY). 2023. PMID: 36821005
References
-
- Sahagun G, Benner KG, Saxon R, et al. Outcome of 100 patients after transjugular intrahepatic portosystemic shunt for variceal hemorrhage. Am J Gastroenterol. 1997;92:1444–1452. - PubMed
LinkOut - more resources
Full Text Sources
