

Awake Glidescope® intubation in a patient with a huge and fixed supraglottic mass -A case report-
- PMID: 21286452
- PMCID: PMC3030048
- DOI: 10.4097/kjae.2010.59.S.S26
Awake Glidescope® intubation in a patient with a huge and fixed supraglottic mass -A case report-
Abstract
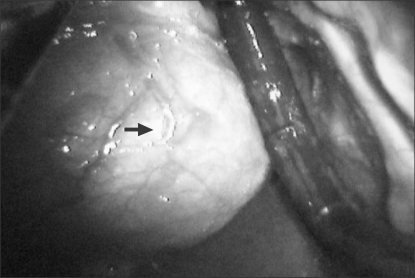
Intubating patients with a huge, fixed supraglottic mass causing an obstruction of the glottis is difficult to most anesthesiologists. We attempted awake fiberoptic orotracheal intubation assisted by Glidescope® Videolaryngoscope (GVL) following topical anesthesia with 4% lidocaine spray and remifentanil infusion. The glottis could not be identified by the GVL view. However, by entering toward the right side of the mass with bronchoscope, the glottis was found. Due to stiffness of the mass, we were unable to further enter the area using the bronchoscope. Alternatively, we attempted to expose the glottis by GVL blade and then successfully intubated the patient by manually pressing the cricoids cartilage. GVL is nonetheless an excellent instrument in airway management compared to fiberoptic bronchoscope for patients with a huge and fixed supraglottic mass.
Keywords: Difficult airway; Fiberoptic bronchoscope; Glidescope; Stylet; Supraglottic mass.
Figures

References
-
- Bradley PJ. Treatment of the patient with upper airway obstruction caused by cancer of the larynx. Otolaryngol Head Neck Surg. 1999;120:737–741. - PubMed
-
- Kanaya N, Nakayama M, Seki S, Kawana S, Watanabe H, Namiki A. Two-person technique for fiberscope-aided tracheal intubation in a patient with a long and narrow retropharyngeal air space. Anesth Analg. 2001;92:1611–1613. - PubMed
-
- Cooper RM, Pacey JA, Bishop MJ, McCluskey SA. Early clinical experience with a new videolaryngoscope (GlideScope) in 728 patients. Can J Anaesth. 2005;52:191–198. - PubMed
-
- Moore MS, Wong AB. GlideScope intubation assisted by fiberoptic scope. Anesthesiology. 2007;106:885. - PubMed
-
- Sukernik MR, Bezinover D, Stahlman B, Vaida S, Pott L. Combination of Glidescope with fiberoptic bronchoscope for the optimization of difficult endotracheal intubation. A case series of three patients. 2009. Jan, Available from http://priory.com/medicine/Glidescope_bronchoscope.htm.
LinkOut - more resources
Full Text Sources
