

Low transition rate from normo- and low microalbuminuria to proteinuria in Japanese type 2 diabetic individuals: the Japan Diabetes Complications Study (JDCS)
- PMID: 21286682
- PMCID: PMC3071947
- DOI: 10.1007/s00125-010-2025-0
Low transition rate from normo- and low microalbuminuria to proteinuria in Japanese type 2 diabetic individuals: the Japan Diabetes Complications Study (JDCS)
Abstract
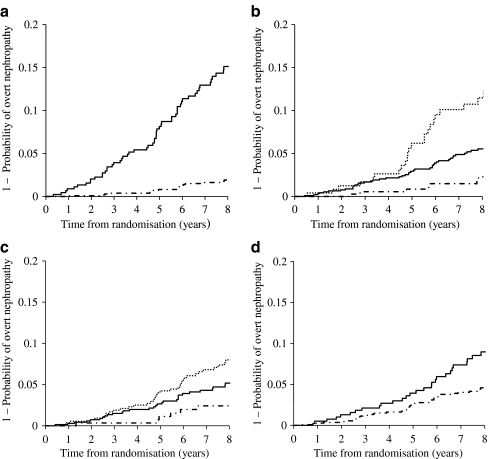
Aims/hypothesis: The aim of the study was to determine the transition rate and factors associated with the progression of normo- and low microalbuminuria to diabetic nephropathy (overt proteinuria).
Methods: For 8 years we prospectively observed 1,558 Japanese patients with type 2 diabetes mellitus whose basal urinary albumin:creatinine ratio (UACR) had been measured as <17.0 mg/mmol at entry. The incidence of nephropathy (UACR >33.9 mg/mmol) was determined by measuring UACR twice a year.
Results: Progression to nephropathy occurred in 74 patients. The annual transition rate was 0.67%, and was substantially higher for the low-microalbuminuric group than for the normoalbuminuric group (1.85% and 0.23%, respectively; hazard ratio for the low-microalbuminuric group 8.45, p < 0.01). The hazard ratio for an HbA(1c) of 7-9% or ≥9% was 2.72 (p < 0.01) or 5.81 (p < 0.01) relative to HbA(1c) <7.0%, respectively. In comparison with individuals with a systolic blood pressure (SBP) of <120 mmHg, the hazard ratios for patients with an SBP of 120-140 mmHg or ≥140 mmHg were 2.31 (p = 0.06) and 3.54 (p < 0.01), respectively. Smoking also affected progression to proteinuria (hazard ratio 1.99, p < 0.01). In contrast, 30.3% of the low-microalbuminuric group returned to normoalbuminuria (i.e. were in remission).
Conclusions/interpretation: These results suggest that if patients with type 2 diabetes mellitus are receiving treatment from diabetologists for hyperglycaemia and hypertension when they are in the early stages of nephropathy (i.e. normo- or low microalbuminuria), their rate of transition to proteinuria is considerably lowered, and that differentiating patients with low microalbuminuria from those with high microalbuminuria might be clinically useful.
Trial registration: UMIN Clinical Trials Registry C000000222.
Figures
References
-
- Statistic Committee of Japan Hemodialysis Society An overview of dialysis treatment in Japan (as of December 31, 2007) J Jpn Hemodialysis Soc. 2009;42:1–45. doi: 10.4009/jsdt.42.1. - DOI
-
- Lui SF, Ho YW, Chu KF, Leung CB, Choy BY. Hong Kong registry 1995–1999. Hong Kong J Nephrol. 1999;1:53–60. doi: 10.1016/S1561-5413(09)60020-X. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
