

Bony increased-offset reversed shoulder arthroplasty: minimizing scapular impingement while maximizing glenoid fixation
- PMID: 21286887
- PMCID: PMC3148388
- DOI: 10.1007/s11999-011-1775-4
Bony increased-offset reversed shoulder arthroplasty: minimizing scapular impingement while maximizing glenoid fixation
Abstract
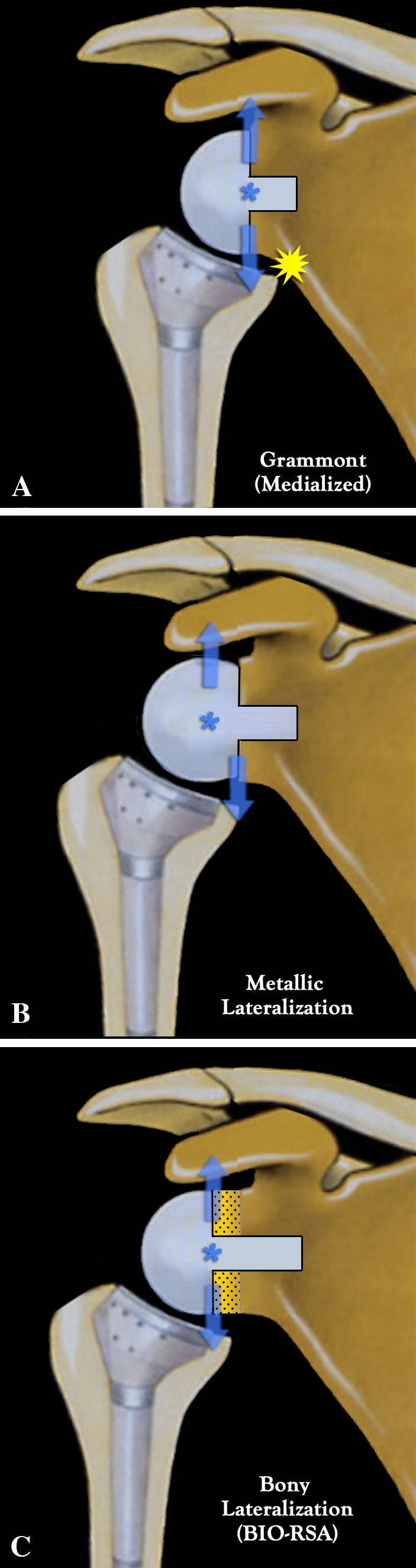
Background: Scapular notching, prosthetic instability, limited shoulder rotation and loss of shoulder contour are associated with conventional medialized design reverse shoulder arthroplasty. Prosthetic (ie, metallic) lateralization increases torque at the baseplate-glenoid interface potentially leading to failure.
Questions/purposes: We asked whether bony lateralization of reverse shoulder arthroplasty would avoid the problems caused by humeral medialization without increasing torque or shear force applied to the glenoid component.
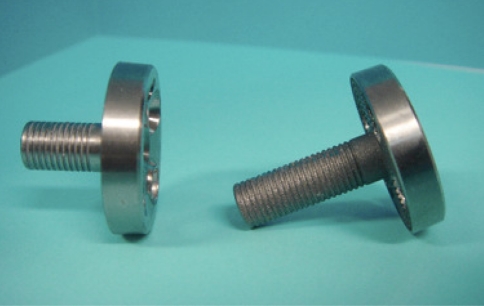
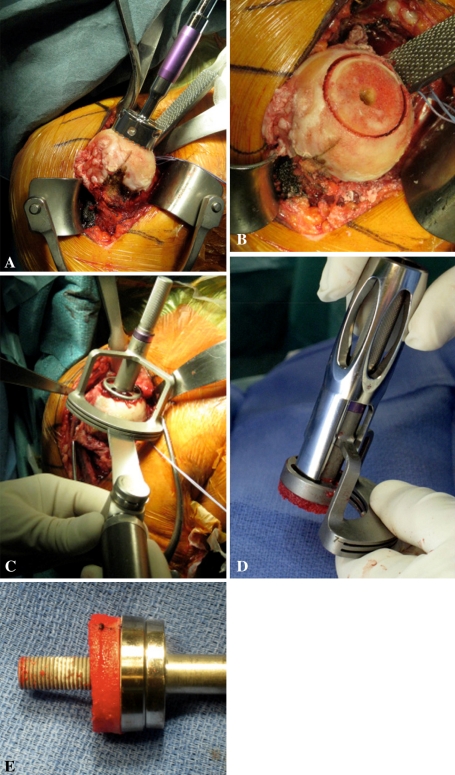
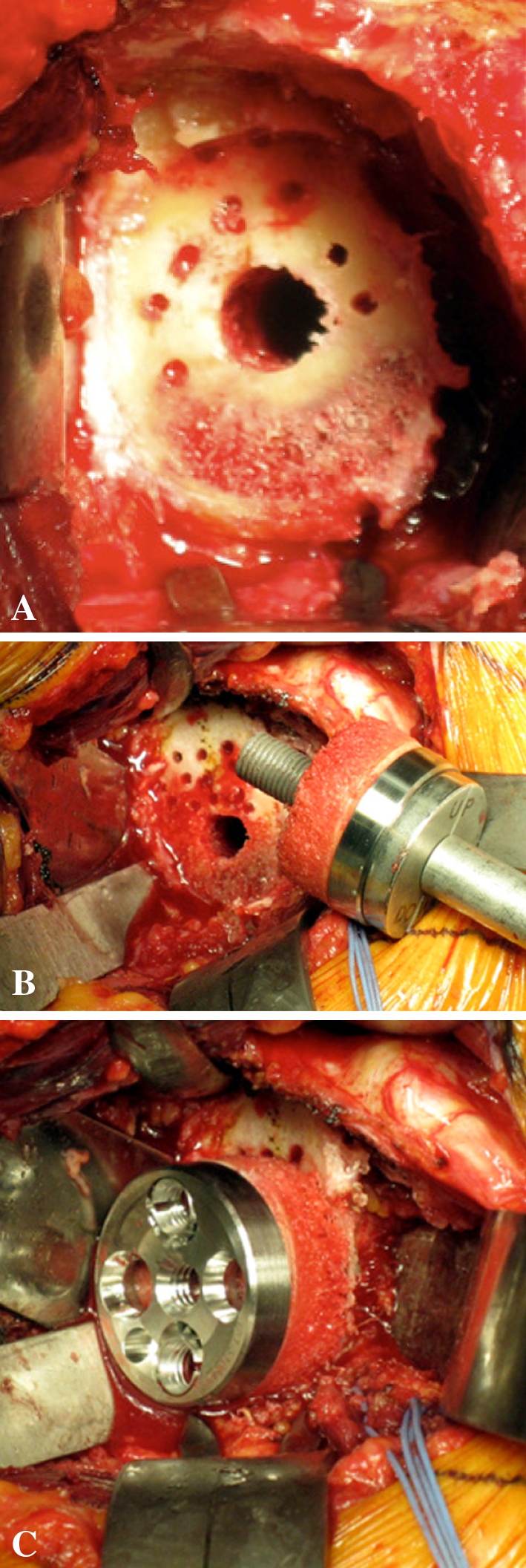
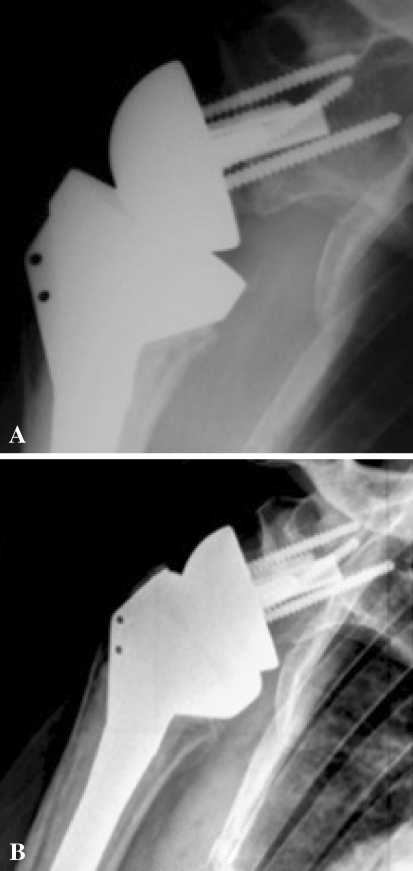
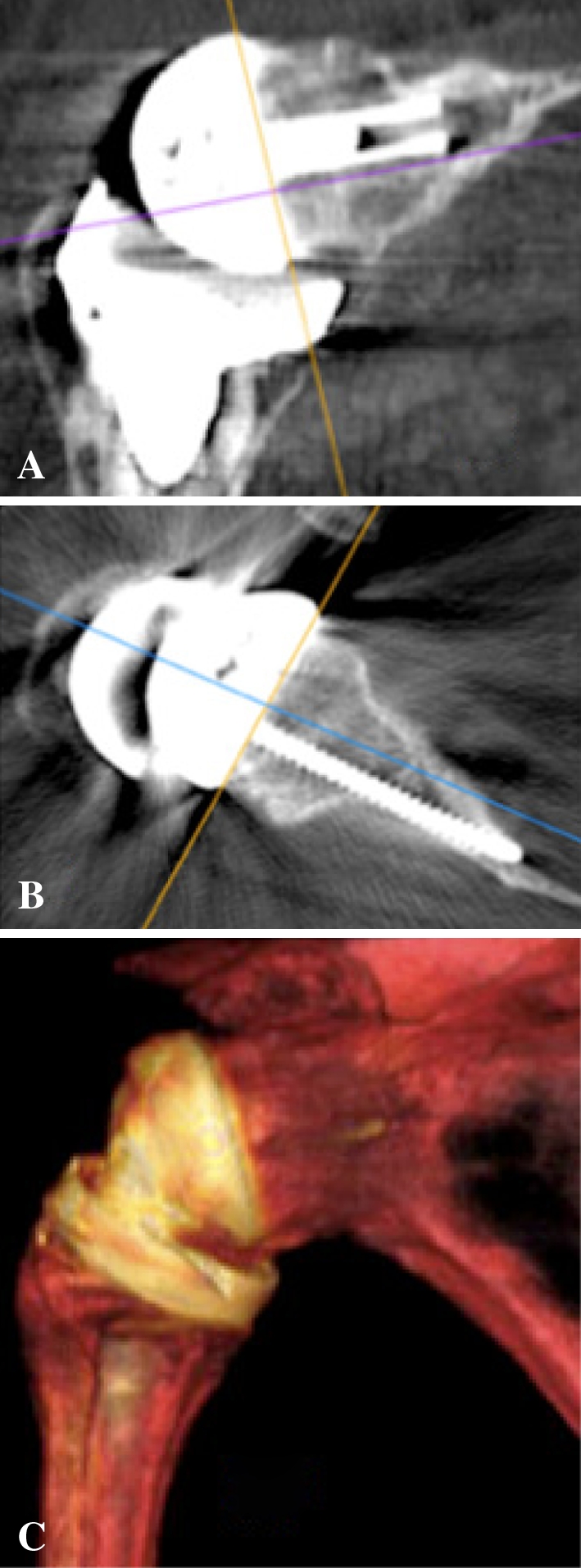
Patients and methods: We prospectively followed 42 patients with rotator cuff deficiency treated with bony increased-offset reverse shoulder arthroplasty. A cylinder of autologous cancellous bone graft, harvested from the humeral head, was placed between the reamed glenoid surface and baseplate. Graft and baseplate fixation was achieved using a lengthened central peg (25 mm) and four screws. Patients underwent clinical, radiographic, and CT assessment at a minimum of 2 years after surgery.
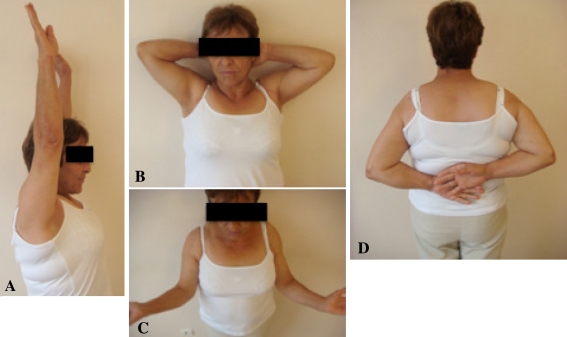
Results: The humeral graft incorporated completely in 98% of cases (41 of 42) and partially in one. At a mean of 28 months postoperatively, no graft resorption, glenoid loosening, or postoperative instability was observed. Inferior scapular notching occurred in 19% (eight of 42). The absolute Constant-Murley score improved from 31 to 67. Thirty-six patients (86%) were able to internally rotate sufficiently to reach their back over the sacrum.
Conclusions: Grafting of the glenoid surface during reverse shoulder arthroplasty effectively creates a long-necked scapula, providing the benefits of lateralization. Bony increased-offset reverse shoulder arthroplasty is associated with low rates of inferior scapular notching, improved shoulder rotation, no prosthetic instability and improved shoulder contour. In contrast to metallic lateralization, bony lateralization has the advantage of maintaining the prosthetic center of rotation at the prosthesis-bone interface, thus minimizing torque on the glenoid component.
Level of evidence: Level IV, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.
Figures
Comment in
-
Bony increased-offset reversed shoulder arthroplasty: minimizing scapular impingement while maximizing glenoid fixation.Clin Orthop Relat Res. 2011 Aug;469(8):2389-90; author reply 2391-2. doi: 10.1007/s11999-011-1926-7. Clin Orthop Relat Res. 2011. PMID: 21660597 Free PMC article. No abstract available.
References
-
- Baulot E, Chabernaud D, Grammont PM. Results of Grammont’s inverted prosthesis in omarthritis associated with major cuff destruction: apropos of 16 cases [in French] Acta Orthop Belg. 1995;61(Suppl 1):112–119. - PubMed
-
- Boileau P, Chuinard C, Roussanne Y, Bicknell RT, Rochet N, Trojani C. Reverse shoulder arthroplasty combined with a modified latissimus dorsi and teres major tendon transfer for shoulder pseudoparalysis associated with dropping arm. Clin Orthop Relat Res. 2008;466:584–593. doi: 10.1007/s11999-008-0114-x. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
