

Intravoxel incoherent motion imaging of tumor microenvironment in locally advanced breast cancer
- PMID: 21287591
- PMCID: PMC4692245
- DOI: 10.1002/mrm.22740
Intravoxel incoherent motion imaging of tumor microenvironment in locally advanced breast cancer
Abstract
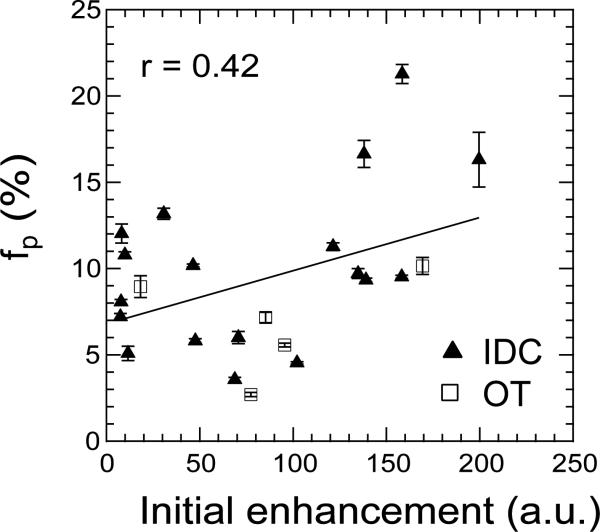
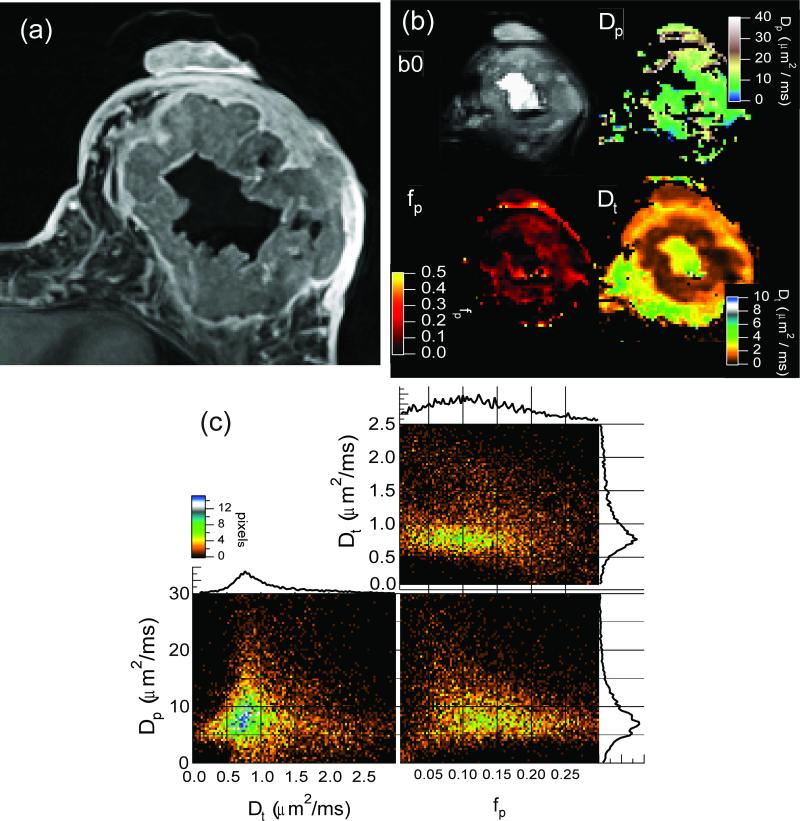
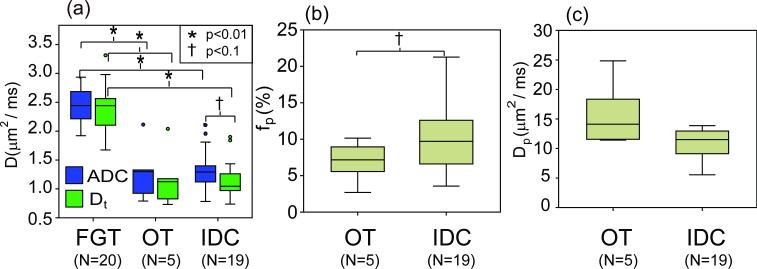
Diffusion-weighted imaging plays important roles in cancer diagnosis, monitoring, and treatment. Although most applications measure restricted diffusion by tumor cellularity, diffusion-weighted imaging is also sensitive to vascularity through the intravoxel incoherent motion effect. Hypervascularity can confound apparent diffusion coefficient measurements in breast cancer. We acquired multiple b-value diffusion-weighted imaging at 3 T in a cohort of breast cancer patients and performed biexponential intravoxel incoherent motion analysis to extract tissue diffusivity (D(t)), perfusion fraction (f(p)), and pseudodiffusivity (D(p)). Results indicated significant differences between normal fibroglandular tissue and malignant lesions in apparent diffusion coefficient mean (±standard deviation) values (2.44 ± 0.30 vs. 1.34 ± 0.39 μm(2)/msec, P < 0.01) and D(t) (2.36 ± 0.38 vs. 1.15 ± 0.35 μm(2)/msec, P < 0.01). Lesion diffusion-weighted imaging signals demonstrated biexponential character in comparison to monoexponential normal tissue. There is some differentiation of lesion subtypes (invasive ductal carcinoma vs. other malignant lesions) with f(p) (10.5 ± 5.0% vs. 6.9 ± 2.9%, P = 0.06), but less so with D(t) (1.14 ± 0.32 μm(2)/msec vs. 1.18 ± 0.52 μm(2)/msec, P = 0.88) and D(p) (14.9 ± 11.4 μm(2)/msec vs. 16.1 ± 5.7 μm(2)/msec, P = 0.75). Comparison of intravoxel incoherent motion biomarkers with contrast enhancement suggests moderate correlations. These results suggest the potential of intravoxel incoherent motion vascular and cellular biomarkers for initial grading, progression monitoring, or treatment assessment of breast tumors.
Copyright © 2010 Wiley-Liss, Inc.
Figures
References
-
- Yamada I, Aung W, Himeno Y, Nakagawa T, Shibuya H. Diffusion Coefficients in Abdominal Organs and Hepatic Lesions: Evaluation with Intravoxel Incoherent Motion Echo-planar MR Imaging. Radiology. 1999;210(3):617–623. - PubMed
-
- Squillaci E, Manenti G, Cova M, Di Roma M, Miano R, Palmieri G, Simonetti G. Correlation of diffusion-weighted MR imaging with cellularity of renal tumours. Anticancer Research. 2004;24(6):4175–4179. - PubMed
-
- McVeigh PZ, Syed AM, Milosevic M, Fyles A, Haider MA. Diffusion-weighted MRI in cervical cancer. European Radiology. 2008;18(5):1058–1064. - PubMed
-
- Sinha S, Sinha U. Functional magnetic resonance of human breast tumors - Diffusion and perfusion imaging. Techniques in Bioinformatics and Medical Informatics. 2002;980:95–115. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
