

First-line antiretroviral therapy with a protease inhibitor versus non-nucleoside reverse transcriptase inhibitor and switch at higher versus low viral load in HIV-infected children: an open-label, randomised phase 2/3 trial
- PMID: 21288774
- PMCID: PMC3111069
- DOI: 10.1016/S1473-3099(10)70313-3
First-line antiretroviral therapy with a protease inhibitor versus non-nucleoside reverse transcriptase inhibitor and switch at higher versus low viral load in HIV-infected children: an open-label, randomised phase 2/3 trial
Abstract
Background: Children with HIV will be on antiretroviral therapy (ART) longer than adults, and therefore the durability of first-line ART and timing of switch to second-line are key questions. We assess the long-term outcome of protease inhibitor and non-nucleoside reverse transcriptase inhibitor (NNRTI) first-line ART and viral load switch criteria in children.
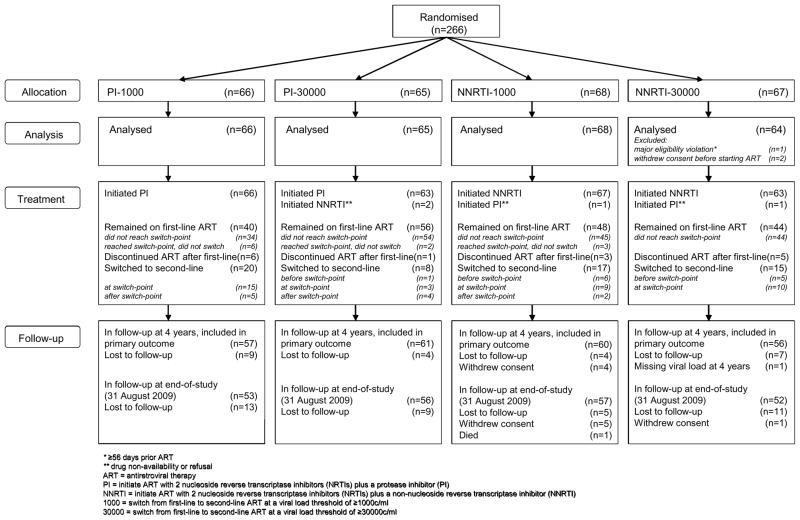
Methods: In a randomised open-label factorial trial, we compared effectiveness of two nucleoside reverse transcriptase inhibitors (NRTIs) plus a protease inhibitor versus two NRTIs plus an NNRTI and of switch to second-line ART at a viral load of 1000 copies per mL versus 30,000 copies per mL in previously untreated children infected with HIV from Europe and North and South America. Random assignment was by computer-generated sequentially numbered lists stratified by age, region, and by exposure to perinatal ART. Primary outcome was change in viral load between baseline and 4 years. Analysis was by intention to treat, which we defined as all patients that started treatment. This study is registered with ISRCTN, number ISRCTN73318385.
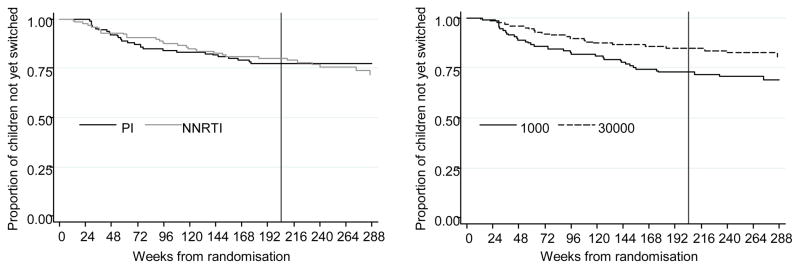
Findings: Between Sept 25, 2002, and Sept 7, 2005, 266 children (median age 6.5 years; IQR 2.8-12.9) were randomly assigned treatment regimens: 66 to receive protease inhibitor and switch to second-line at 1000 copies per mL (PI-low), 65 protease inhibitor and switch at 30,000 copies per mL (PI-higher), 68 NNRTI and switch at 1000 copies per mL (NNRTI-low), and 67 NNRTI and switch at 30,000 copies per mL (NNRTI-higher). Median follow-up was 5.0 years (IQR 4.2-6.0) and 188 (71%) children were on first-line ART at trial end. At 4 years, mean reductions in viral load were -3.16 log(10) copies per mL for protease inhibitors versus -3.31 log(10) copies per mL for NNRTIs (difference -0.15 log(10) copies per mL, 95% CI -0.41 to 0.11; p=0.26), and -3.26 log(10) copies per mL for switching at the low versus -3.20 log(10) copies per mL for switching at the higher threshold (difference 0.06 log(10) copies per mL, 95% CI -0.20 to 0.32; p=0.56). Protease inhibitor resistance was uncommon and there was no increase in NRTI resistance in the PI-higher compared with the PI-low group. NNRTI resistance was selected early, and about 10% more children accumulated NRTI mutations in the NNRTI-higher than the NNRTI-low group. Nine children had new CDC stage-C events and 60 had grade 3/4 adverse events; both were balanced across randomised groups.
Interpretation: Good long-term outcomes were achieved with all treatments strategies. Delayed switching of protease-inhibitor-based ART might be reasonable where future drug options are limited, because the risk of selecting for NRTI and protease-inhibitor resistance is low.
Funding: Paediatric European Network for Treatment of AIDS (PENTA) and Pediatric AIDS Clinical Trials Group (PACTG/IMPAACT).
Copyright © 2011 Elsevier Ltd. All rights reserved.
Conflict of interest statement
SF received honoraria for serving on Scientific Advisory Boards and/or lectures from Abbott Molecular Inc and Roche Molecular Systems. MH is a paid Data and Safety Monitoring Board member for Boehringer Ingelheim, Medicines Development, Pfizer and Tibotec. RM is a paid Data and Safety Monitoring Board member for Gilead Sciences. DMG and ASW are paid Data and Safety Monitoring Board members for Tibotec. No other member of the Writing Committee has a conflict of interest.
Figures

Comment in
-
ART for children: what to start and when to switch.Lancet Infect Dis. 2011 Apr;11(4):254-5. doi: 10.1016/S1473-3099(11)70004-4. Epub 2011 Jan 31. Lancet Infect Dis. 2011. PMID: 21288775 No abstract available.
References
-
- Palella FJ, Jr, Delaney KM, Moorman AC, Loveless MO, Fuhrer J, Satten GA, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med. 1998 Mar 26;338(13):853–60. - PubMed
-
- Vigouroux C, Gharakhanian S, Salhi Y, Nguyen TH, Adda N, Rozenbaum W, et al. Adverse metabolic disorders during highly active antiretroviral treatments (HAART) of HIV disease. Diabetes Metab. 1999 Nov;25(5):383–92. - PubMed
-
- Faye A, Bertone C, Teglas JP, Chaix ML, Douard D, Firtion G, et al. Early multitherapy including a protease inhibitor for human immunodeficiency virus type 1-infected infants. Pediatr Infect Dis J. 2002 Jun;21(6):518–25. - PubMed
-
- Luzuriaga K, McManus M, Mofenson L, Britto P, Graham B, Sullivan JL. A trial of three antiretroviral regimens in HIV-1-infected children. N Engl J Med. 2004 Jun 10;350(24):2471–80. - PubMed
-
- Funk MB, Linde R, Wintergerst U, Notheis G, Hoffmann F, Schuster T, et al. Preliminary experiences with triple therapy including nelfinavir and two reverse transcriptase inhibitors in previously untreated HIV-infected children. AIDS. 1999 Sep 10;13(13):1653–8. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- HHSN267200800001G/DK/NIDDK NIH HHS/United States
- G0400858/MRC_/Medical Research Council/United Kingdom
- HHSN267200800001C/DK/NIDDK NIH HHS/United States
- U01 AI068632/AI/NIAID NIH HHS/United States
- UM1 AI068632/AI/NIAID NIH HHS/United States
- UM1 AI069415/AI/NIAID NIH HHS/United States
- MC_U122886353/MRC_/Medical Research Council/United Kingdom
- U01 AI068616/AI/NIAID NIH HHS/United States
- HHSN267200800001C/HD/NICHD NIH HHS/United States
- U01 AI041110/AI/NIAID NIH HHS/United States
- N01-DK-9-001/HHSN267200800001C/DK/NIDDK NIH HHS/United States
- AI068632/AI/NIAID NIH HHS/United States
- 1 U01 AI068616/AI/NIAID NIH HHS/United States
- 5 U01 AI41110/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
