

Surgical resection and survival of patients with unsuspected single node positive lung cancer (NSCLC) invading the descending aorta
- PMID: 21289904
- PMCID: PMC3011294
- DOI: 10.3205/tss000016
Surgical resection and survival of patients with unsuspected single node positive lung cancer (NSCLC) invading the descending aorta
Abstract
Background: Surgical treatment of non-small cell lung cancer (NSCLC) with aortic invasion is still debated.
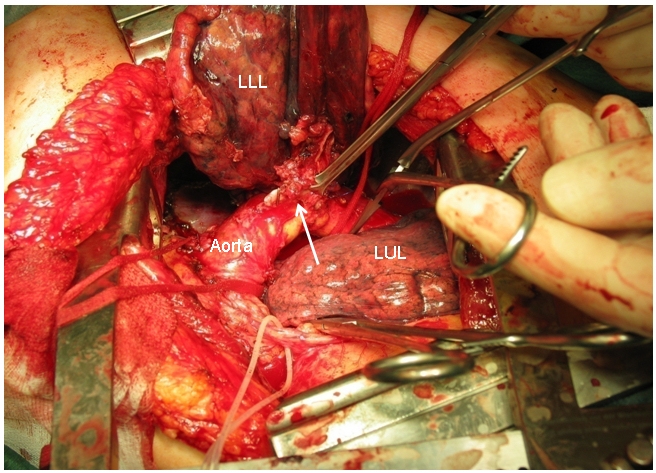
Methods: Thirteen patients with locally advanced (T4) NSCLC and invasion of the descending aorta underwent pneumonectomy (n=9) or lobectomy (n=4) together with aorta en bloc resection and reconstruction (n=8) or subadventitial dissection (n=5), complete lymph node dissection, and had microscopic unsuspected node metastasis at N1 (n=5) and N2/3 (n=8) levels of whom 12 received radiation therapy. Clamp-and-sew was used to resect and reconstruct the aorta.
Results: Operative mortality and morbidity rate was 0% and 23%, respectively. Four patients died of systemic tumor relapse and 2 of local recurrence. Six patients were alive after a median follow-up of 40 months (range 15-125 months). Overall 5-year survival rate was 45%. Median survival time and 5-year survival rate of patients after aortic resection was 35 months and 67%, respectively, and was 17 months and 0%, respectively, after aortic subadventi-tial dissection (p=0.001). N1 and N2 nodal status adversely affected survival, but survival difference was not significant (N1 versus N2/3; 52% versus 39% at 5 years; p=0.998).
Conclusions: Aortic resection with single station node positive T4 lung cancer can achieve long-term survival. The data indicate that aortic resection-reconstruction is associated with better outcome than subadventitial dissection.
Hintergrund: Die chirurgische Behandlung nicht-kleinzelliger Lungentumore mit Aortawandinvasion wird kontrovers diskutiert.
Methoden: 13 Patienten mit lokal fortgeschrittenem (T4) nicht-kleinzelligen Lungencarcinom, tumoröser Invasion der Aorta descendens und präoperativ negativem N-Staging wurden in kurativer Intention primär operiert. Operative Prozeduren: Pneumonektomie 8-mal, Lobektomie 4-mal in Kombination mit segmental aortaler en-bloc-Resektion „clamp-and-sew“ in 8 Fällen oder subadventitieller Aortawanddissektion in 5 Fällen und systematischer Lymphknotendissektion. 12 Patienten mit definitiv solitärer, mikroskopischer Lymphknotenmetastase in N1- (n=5) oder N2-Position (n=8) erhielten eine adjuvante Radiotherapie.
Ergebnisse: Die Krankenhaus-, resp. 90-Tage-Mortalität betrug 0%, die Morbidität 23%. Im weiteren Verlauf verstarben 4 Patienten an disseminierter Metastasierung und 2 Patienten am lokalen Tumorrezidiv. Bei einem mittleren Nachbeobachtungszeitraum von 40 Monaten leben noch 6 Patienten (15–125 Monate). Die kumulativ prospektive 5-Jahresüberlebensrate der 13 Patienten betrug 45%. Die mittlere Überlebenszeit und 5-Jahresüberlebensrate nach Aortaresektion betrug 35 Monate und 67%, nach Aortawanddissektion respektive 17 Monate und 0% (p=0,001). Der N1- und N2/3-Lymphknotenstatus beeinträchtigten das Langzeitüberleben (N1 versus N2/3; 52% versus 39% nach 5 Jahren). Der Überlebensunterschied erreichte kein Signifikanzniveau (p=0,998).
Schlussfolgerungen: Bei einer lokal fortgeschrittenen Lungenkrebserkrankung ist in ausgewählten Fällen, auch bei Vorliegen einer solitären Lymphknotenmetastase, mit einer primären, erweiterten Resektionstherapie ein Langzeitüberleben erzielbar. Nach unseren Ergebnissen ist bei umschriebener aortaler Infiltration der aortalen en-bloc-Resektion gegenüber der subadventitiellen Aortawanddissektion der Vorzug zu geben. Weitere Studien sollten den Nutzen multimodaler Therapiekonzepte evaluieren.
Keywords: aortic operation; lung cancer surgery; off pump; outcomes.
Figures








Similar articles
-
Surgery for T4 lung cancer invading the thoracic aorta: Do we push the limits?J Surg Oncol. 2017 Dec;116(8):1141-1149. doi: 10.1002/jso.24784. Epub 2017 Sep 18. J Surg Oncol. 2017. PMID: 28922454
-
Lobectomy does not confer survival advantage over segmentectomy for non-small cell lung cancer with unsuspected nodal disease.J Thorac Cardiovasc Surg. 2020 Jun;159(6):2469-2483.e4. doi: 10.1016/j.jtcvs.2019.10.165. Epub 2019 Nov 21. J Thorac Cardiovasc Surg. 2020. PMID: 31928821
-
Factors affecting long-term survival after en-bloc resection of lung cancer invading the chest wall.Eur J Cardiothorac Surg. 2000 Nov;18(5):513-8. doi: 10.1016/s1010-7940(00)00537-6. Eur J Cardiothorac Surg. 2000. PMID: 11053809
-
The present status of surgery for lung cancer.Acta Chir Belg. 1996 Nov-Dec;96(6):245-51. Acta Chir Belg. 1996. PMID: 9008764 Review.
-
Oncological outcomes of unsuspected pN2 in patients with non-small-cell lung cancer: a systematic review and meta-analysis.Interact Cardiovasc Thorac Surg. 2021 May 10;32(5):727-736. doi: 10.1093/icvts/ivaa334. Interact Cardiovasc Thorac Surg. 2021. PMID: 33517373 Free PMC article.
Cited by
-
T4 Lung Carcinoma with Infiltration of the Thoracic Aorta: Indication and Surgical Procedure.Cancers (Basel). 2023 Oct 4;15(19):4847. doi: 10.3390/cancers15194847. Cancers (Basel). 2023. PMID: 37835540 Free PMC article. Review.
-
Initial extended resection or neoadjuvant therapy for T4 non-small cell lung cancer-What is the evidence?Shanghai Chest. 2018 Oct;2:76. doi: 10.21037/shc.2018.09.08. Epub 2018 Oct 11. Shanghai Chest. 2018. PMID: 30498811 Free PMC article.
-
Long-term survival in locally advanced non-small cell lung cancer invading the great vessels and heart.Thorac Cancer. 2018 May;9(5):598-605. doi: 10.1111/1759-7714.12625. Epub 2018 Mar 30. Thorac Cancer. 2018. PMID: 29602232 Free PMC article.
-
Synchronous Multiple Primary Cancers of the Lung: The Rare Association of Non-Small Cell Carcinoma With a Carcinoid Tumor.Cureus. 2020 Aug 20;12(8):e9888. doi: 10.7759/cureus.9888. Cureus. 2020. PMID: 32968554 Free PMC article.
-
T4-non-small cell lung cancer invading the thoracic aorta: the role of the hybrid operating room.J Thorac Dis. 2025 Jan 24;17(1):496-502. doi: 10.21037/jtd-24-1724. Epub 2025 Jan 21. J Thorac Dis. 2025. PMID: 39975741 Free PMC article.
References
-
- Burt ME, Pomerantz AH, Bains MS, McCormack PM, Kaiser LR, Hilaris BS, Martini N. Results of surgical treatment of stage III lung cancer invading the mediastinum. Surg Clin North Am. 1987;67(5):987–1000. - PubMed
-
- Martini N, Yellin A, Ginsberg RJ, Bains MS, Burt ME, McCormack PM, Rusch VW. Management of non-small cell lung cancer with direct mediastinal involvement. Ann Thorac Surg. 1994;58(5):1447–1451. - PubMed
-
- Dartevelle PG. Herbert Sloan Lecture. Extended operations for the treatment of lung cancer. Ann Thorac Surg. 1997;63(1):12–19. - PubMed
-
- Rice TW, Blackstone EH. Radical resections for T4 lung cancer. Surg Clin North Am. 2002;82(3):573–587. doi: 10.1016/S0039-6109(02)00017-8. Available from: http://dx.doi.org/10.1016/S0039-6109(02)00017-8. - DOI - DOI - PubMed
-
- Cerfolio RJ, Bryant AS. Survival of patients with unsuspected N2 (stage IIIA) nonsmall-cell lung cancer. Ann Thorac Surg. 2008;86(2):362–366. doi: 10.1016/j.athoracsur.2008.04.042. Available from: http://dx.doi.org/10.1016/j.athoracsur.2008.04.042. - DOI - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
