

Comparable efficacy and safety of insulin glulisine and insulin lispro when given as part of a Basal-bolus insulin regimen in a 26-week trial in pediatric patients with type 1 diabetes
- PMID: 21291333
- PMCID: PMC3045789
- DOI: 10.1089/dia.2010.0072
Comparable efficacy and safety of insulin glulisine and insulin lispro when given as part of a Basal-bolus insulin regimen in a 26-week trial in pediatric patients with type 1 diabetes
Abstract
Background: We compared the efficacy and safety of insulin glulisine with insulin lispro as part of a basal-bolus regimen in children and adolescents with type 1 diabetes.
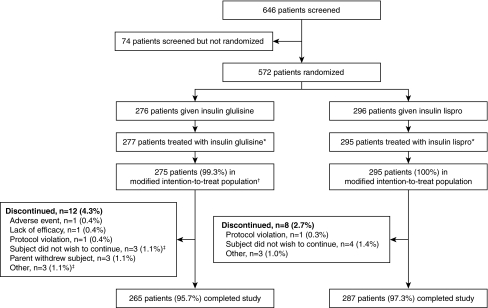
Methods: Overall, 572 children and adolescents (4-17 years old) using insulin glargine or neutral protamine Hagedorn insulin as basal insulin were enrolled in a 26-week, multicenter, open, centrally randomized, parallel-group, noninferiority study. Subjects were randomized to receive glulisine (n = 277) or lispro (n= 295) 0-15 min premeal.
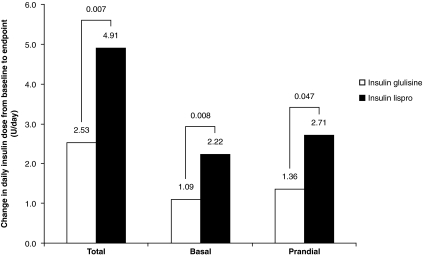
Results: Baseline-to-endpoint hemoglobin A1c changes were similar between the two insulins: adjusted mean change (glulisine vs. lispro), 0.10% versus 0.16%; between-treatment difference (glulisine-lispro), &minsu;0.06, 95% confidence interval (-0.24; 0.12); and prespecified noninferiority margin, 0.4%. Overall, for all age groups together, the percentage of patients achieving American Diabetes Association age-specific A1c targets at endpoint was significantly higher (P = 0.039) with glulisine (38.4%) versus lispro (32.0%). From Month 4 to endpoint, both "all" and "severe" symptomatic hypoglycemia rates were similar (3.10 vs. 2.91 and 0.06 vs. 0.07 events/patient-month, respectively). Frequency and type of adverse events, serious adverse events, or hypoglycemia reported as serious adverse events were similar between both groups.
Conclusions: Glulisine was as effective as lispro in baseline-to-endpoint A1c change, and both treatments were similarly well tolerated.
Figures
References
-
- Rewers M. Pihoker C. Donaghue K. Hanas R. Swift P. Klingensmith GJ. Assessment and monitoring of glycemic control in children and adolescents with diabetes. Pediatr Diabetes. 2009;10:71–81. - PubMed
-
- American Diabetes Association: Standards of medical care in diabetes—2006. Diabetes Care. 2006;29(Suppl 1):S4–S42. Erratum in: Diabetes Care 2006;29:1192. - PubMed
-
- Koivisto VA. The human insulin analogue insulin lispro. Ann Med. 1998;30:260–266. - PubMed
-
- Lindholm A. Jacobsen LV. Clinical pharmacokinetics and pharmacodynamics of insulin aspart. Clin Pharmacokinet. 2001;40:641–659. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical