

Beat-to-beat respiratory motion correction with near 100% efficiency: a quantitative assessment using high-resolution coronary artery imaging
- PMID: 21292418
- PMCID: PMC3082051
- DOI: 10.1016/j.mri.2010.11.004
Beat-to-beat respiratory motion correction with near 100% efficiency: a quantitative assessment using high-resolution coronary artery imaging
Abstract
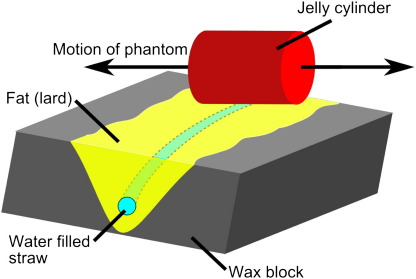
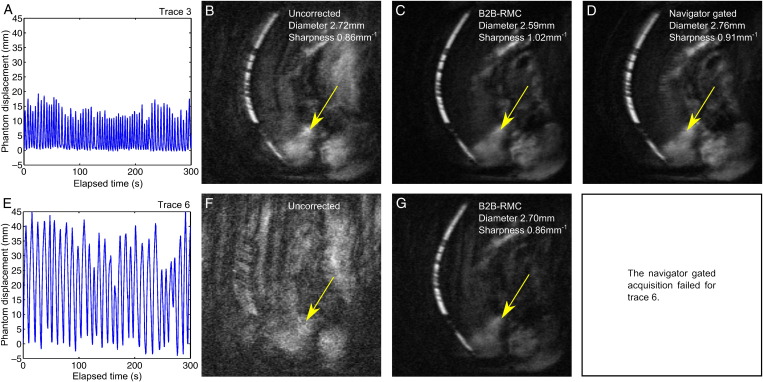
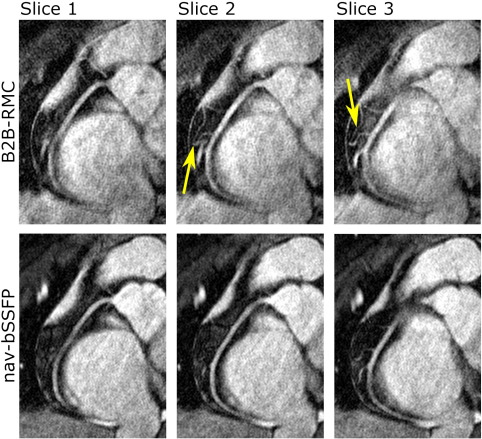
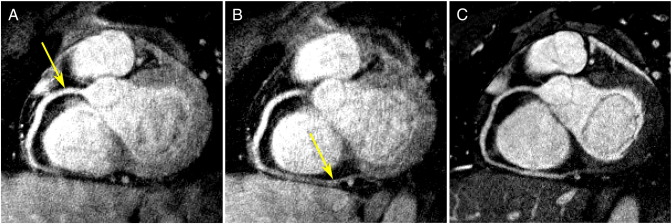
This study quantitatively assesses the effectiveness of retrospective beat-to-beat respiratory motion correction (B2B-RMC) at near 100% efficiency using high-resolution coronary artery imaging. Three-dimensional (3D) spiral images were obtained in a coronary respiratory motion phantom with B2B-RMC and navigator gating. In vivo, targeted 3D coronary imaging was performed in 10 healthy subjects using B2B-RMC spiral and navigator gated balanced steady-state free-precession (nav-bSSFP) techniques. Vessel diameter and sharpness in proximal and mid arteries were used as a measure of respiratory motion compensation effectiveness and compared between techniques. Phantom acquisitions with B2B-RMC were sharper than those acquired with navigator gating (B2B-RMC vs. navigator gating: 1.01±0.02 mm(-1) vs. 0.86±0.08 mm(-1), P<.05). In vivo B2B-RMC respiratory efficiency was significantly and substantially higher (99.7%±0.5%) than nav-bSSFP (44.0%±8.9%, P<.0001). Proximal and mid vessel sharpnesses were similar (B2B-RMC vs. nav-bSSFP, proximal: 1.00±0.14 mm(-1) vs. 1.08±0.11 mm(-1), mid: 1.01±0.11 mm(-1) vs. 1.05±0.12 mm(-1); both P=not significant [ns]). Mid vessel diameters were not significantly different (2.85±0.39 mm vs. 2.80±0.35 mm, P=ns), but proximal B2B-RMC diameters were slightly higher (2.85±0.38 mm vs. 2.70±0.34 mm, P<.05), possibly due to contrast differences. The respiratory efficiency of B2B-RMC is less variable and significantly higher than navigator gating. Phantom and in vivo vessel sharpness and diameter values suggest that respiratory motion compensation is equally effective.
Copyright © 2011 Elsevier Inc. All rights reserved.
Figures
References
-
- Danias P.G., McConnell M.V., Khasgiwala V.C., Chuang M.L., Edelman R.R., Manning W.J. Prospective navigator correction of image position for coronary MR angiography. Radiology. 1997;203(3):733–736. - PubMed
-
- Ehman R.L., Felmlee J.P. Adaptive technique for high-definition MR imaging of moving structures. Radiology. 1989;173(1):255–263. - PubMed
-
- Sachs T.S., Meyer C.H., Hu B.S., Kohli J., Nishimura D.G., Macovski A. Real-time motion detection in spiral MRI using navigators. Magn Reson Med. 1994;32(5):639–645. - PubMed
-
- Oshinski J.N., Hofland L., Mukundan S., Dixon W.T., Parks W.J., Pettigrew R.I. Two-dimensional coronary MR angiography without breath holding. Radiology. 1996;201(3):737–743. - PubMed
-
- Taylor A.M., Jhooti P., Wiesmann F., Keegan J., Firmin D.N., Pennell D.J. MR navigator-echo monitoring of temporal changes in diaphragm position: implications for MR coronary angiography. J Magn Reson Imaging. 1997;7(4):629–636. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
