

Early cost and safety benefits of an inpatient electronic health record
- PMID: 21292703
- PMCID: PMC3116263
- DOI: 10.1136/jamia.2010.007229
Early cost and safety benefits of an inpatient electronic health record
Abstract
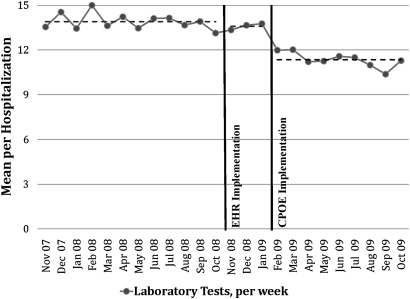
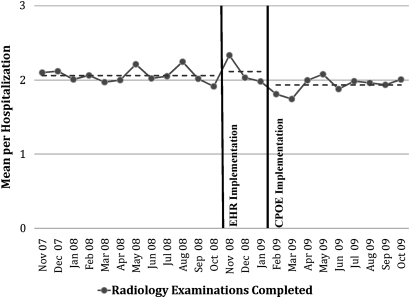
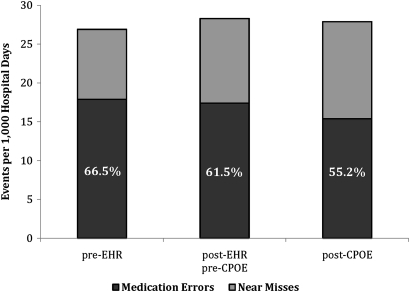
There is controversy over the impact of electronic health record (EHR) systems on cost of care and safety. The authors studied the effects of an inpatient EHR system with computerized provider order entry on selected measures of cost of care and safety. Laboratory tests per week per hospitalization decreased from 13.9 to 11.4 (18%; p < 0.001). Radiology examinations per hospitalization decreased from 2.06 to 1.93 (6.3%; p < 0.009). Monthly transcription costs declined from $74,596 to $18,938 (74.6%; p < 0.001). Reams of copy paper ordered per month decreased from 1668 to 1224 (26.6%; p < 0.001). Medication errors per 1000 hospital days decreased from 17.9 to 15.4 (14.0%; p < 0.030), while near misses per 1000 hospital days increased from 9.0 to 12.5 (38.9%; p < 0.037), and the percentage of medication events that were medication errors decreased from 66.5% to 55.2% (p < 0.007). In this manuscript, we demonstrate that the implementation of an inpatient EHR with computerized provider order entry can result in rapid improvement in measures of cost of care and safety.
Conflict of interest statement
Figures
References
-
- Centers for Medicare and Medicaid Services Medicare and Medicaid Programs; Electronic Health Record Incentive Program; Proposed Rule. http://www.cms.gov/Recovery/Downloads/CMS-2009-0117-0002.pdf (accessed 28 Apr 2010).
-
- Kohn LT, Corrigan JM, Donaldson MS. To Err is Human: Building a safer Health System. Washington, D.C: Institute of Medicine, National Academy Press, 1999 - PubMed
-
- Milstein A, Galvin RS, Delbanco SF, et al. Improving the safety of health care: the leapfrog initiative. Eff Clin Pract 2000;3:313–16 - PubMed
-
- Walker J, Pan E, Johnston D, et al. The Value of Health Care Information Exchange and Interoperability. Health Aff, Millwood, 2005. http://content.healthaffairs.org/cgi/content/full/hlthaff.w5.10/DC1 (accessed 29 Jun 2010). - PubMed
-
- Girosi F, Meili R, Scoville RP. Extrapolating Evidence of Health Information Technology Savings and Costs. Santa Monica, CA: RAND Health, 2005:94 http://www.rand.org/pubs/monographs/2005/RAND_MG410.pdf (accessed 29 Jun 2010).
