

Code status orders and goals of care in the medical ICU
- PMID: 21292755
- PMCID: PMC3198491
- DOI: 10.1378/chest.10-1798
Code status orders and goals of care in the medical ICU
Abstract
Background: Decisions about CPR in the medical ICU (MICU) are important. However, discussions about CPR (code status discussions) can be challenging and may be incomplete if they do not address goals of care.
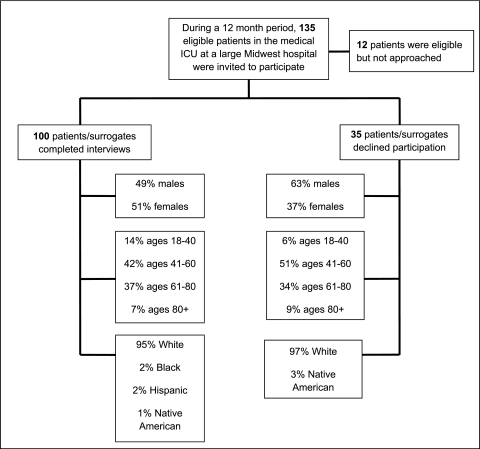
Methods: We interviewed 100 patients, or their surrogates, and their physicians in an MICU. We queried the patients/surrogates on their knowledge of CPR, code status preferences, and goals of care; we queried MICU physicians about goals of care and treatment plans. Medical records were reviewed for clinical information and code status orders.
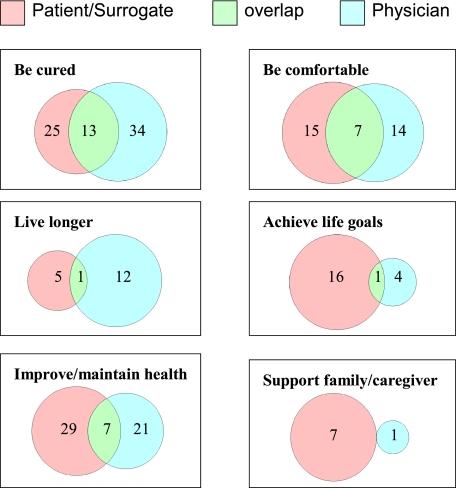
Results: Fifty patients/surrogates recalled discussing CPR preferences with a physician, and 51 recalled discussing goals of care. Eighty-three patients/surrogates preferred full code status, but only four could identify the three main components of in-hospital CPR (defibrillation, chest compressions, intubation). There were 16 discrepancies between code status preferences expressed during the interview and code status orders in the medical record. Respondents' average prediction of survival following in-hospital cardiac arrest with CPR was 71.8%, and the higher the prediction of survival, the greater the frequency of preference for full code status (P = .012). Of six possible goals of care, approximately five were affirmed by each patient/surrogate and physician, but 67.7% of patients/surrogates differed with their physicians about the most important goal of care.
Conclusions: Patients in the MICU and their surrogates have inadequate knowledge about in-hospital CPR and its likelihood of success, patients' code status preferences may not always be reflected in code status orders, and assessments may differ between patients/surrogates and physicians about what goal of care is most important.
Figures
Comment in
-
The language of goals of care: framing preferences at the end of life.Chest. 2012 Apr;141(4):1126. doi: 10.1378/chest.11-2883. Chest. 2012. PMID: 22474163 No abstract available.
References
-
- von Gunten CF, Ferris FD, Emanuel LL. The patient-physician relationship. Ensuring competency in end-of-life care: communication and relational skills. JAMA. 2000;284(23):3051–3057. - PubMed
-
- Hofmann JC, Wenger NS, Davis RB, et al. SUPPORT Investigators. Study to Understand Prognoses and Preference for Outcomes and Risks of Treatment Patient preferences for communication with physicians about end-of-life decisions. Ann Intern Med. 1997;127(1):1–12. - PubMed
-
- Wenger NS, Phillips RS, Teno JM, et al. Physician understanding of patient resuscitation preferences: insights and clinical implications. J Am Geriatr Soc. 2000;48(5) Suppl:S44–S51. - PubMed
-
- White DB, Braddock CH, III, Bereknyei S, Curtis JR. Toward shared decision making at the end of life in intensive care units: opportunities for improvement. Arch Intern Med. 2007;167(5):461–467. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
