

Contribution of adenosine to compensatory dilation in hypoperfused contracting human muscles is independent of nitric oxide
- PMID: 21292838
- PMCID: PMC3098657
- DOI: 10.1152/japplphysiol.00836.2010
Contribution of adenosine to compensatory dilation in hypoperfused contracting human muscles is independent of nitric oxide
Abstract
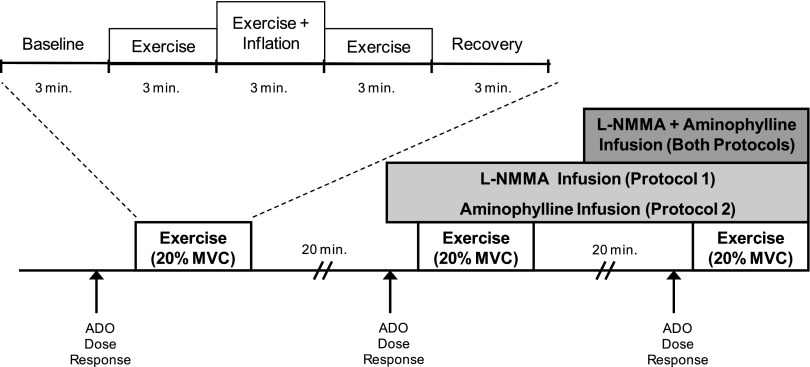
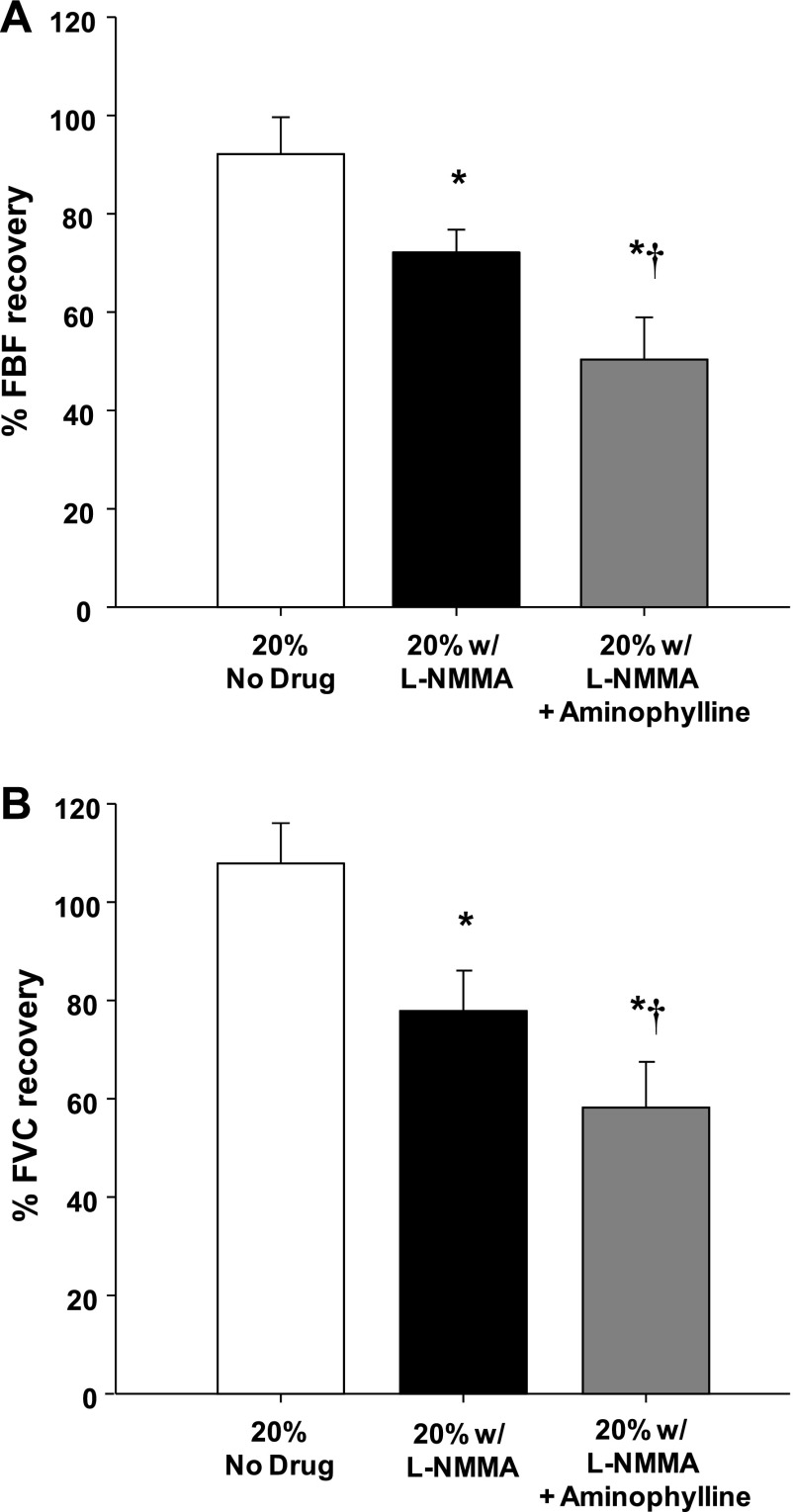
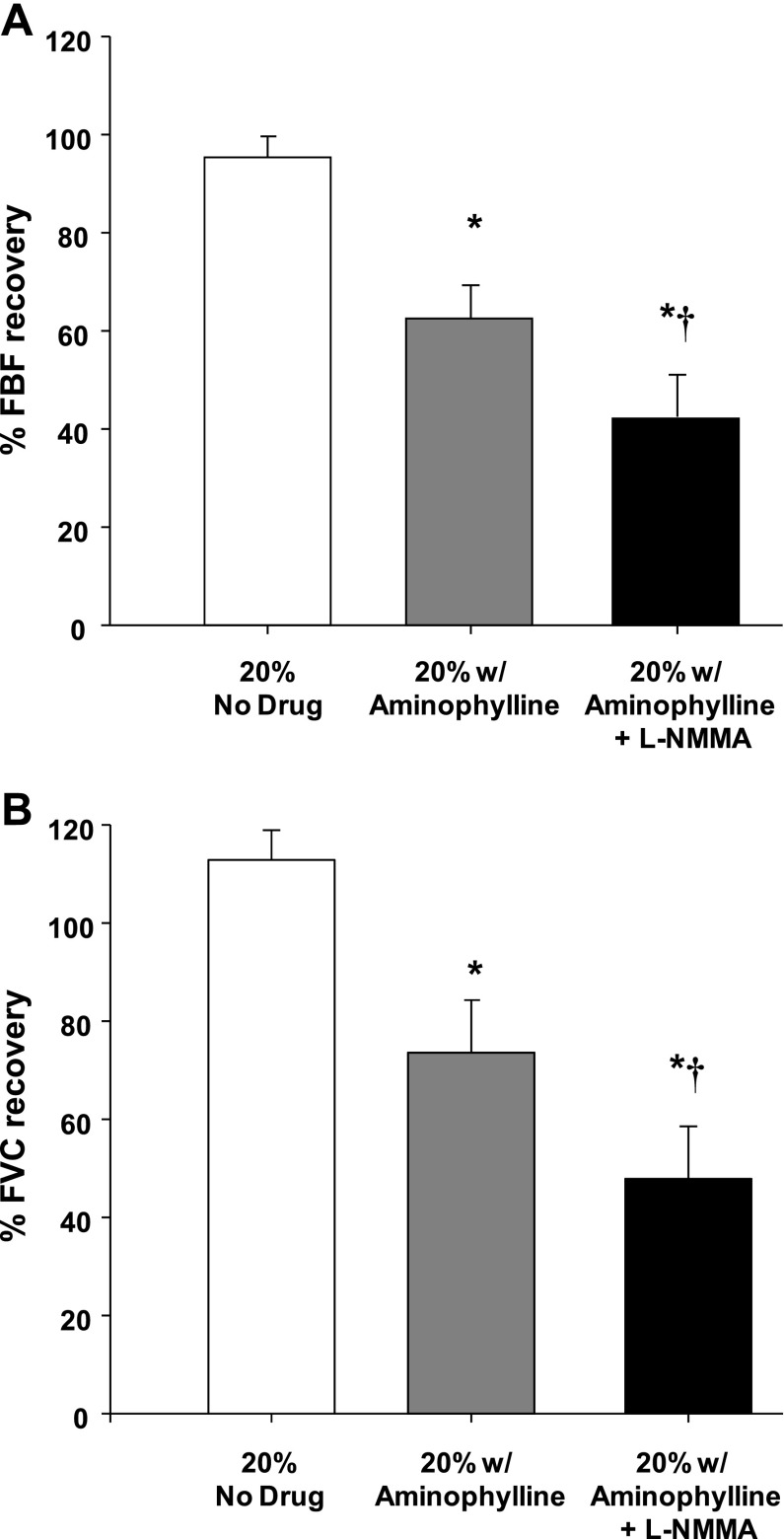
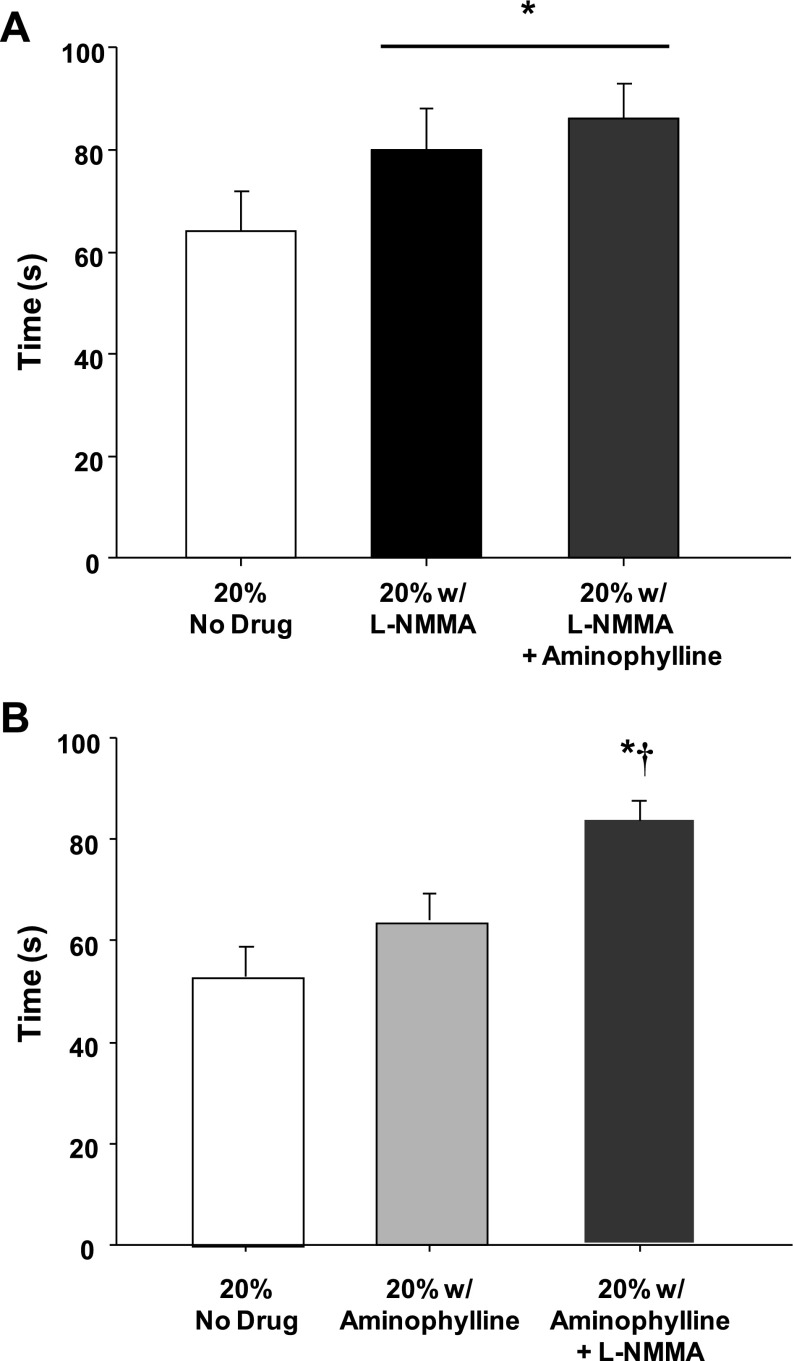
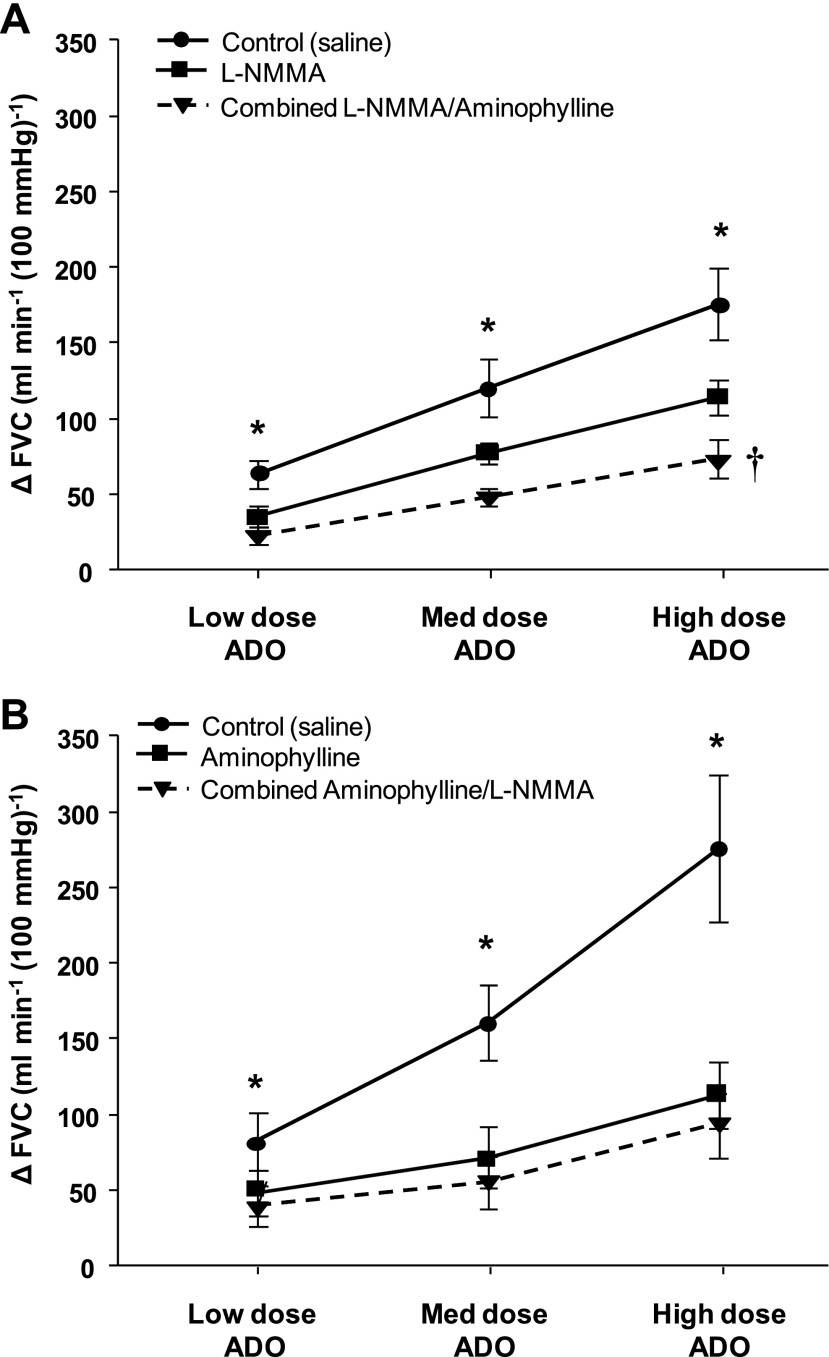
We previously demonstrated that nitric oxide (NO) contributes to compensatory vasodilation in the contracting human forearm subjected to acute hypoperfusion. We examined the potential role of an adenosine-NO interaction to this response in 17 male subjects (25 ± 2 yr). In separate protocols subjects performed rhythmic forearm exercise (20% of maximum) while hypoperfusion was evoked by balloon inflation in the brachial artery above the elbow. Each trial included exercise before inflation, exercise with inflation, and exercise after deflation (3 min each). Forearm blood flow (FBF; ultrasound) and local [brachial artery catheter pressure (BAP)] and systemic [mean arterial pressure (MAP); Finometer] arterial pressure were measured. In protocol 1 (n = 10), exercise was repeated during nitric oxide synthase inhibition [N(G)-monomethyl-L-arginine (L-NMMA)] alone and during L-NMMA-aminophylline (adenosine receptor blockade) administration. In protocol 2, exercise was repeated during aminophylline alone and during aminophylline-L-NMMA. Forearm vascular conductance (FVC; ml·min(-1)·100 mmHg(-1)) was calculated from blood flow (ml/min) and BAP (mmHg). Percent recovery in FVC during inflation was calculated as (steady-state inflation + exercise value - nadir)/[steady-state exercise (control) value - nadir]. In protocol 1, percent recovery in FVC was 108 ± 8% during the control (no drug) trial. Percent recovery in FVC was attenuated with inhibition of NO formation alone (78 ± 9%; P < 0.01 vs. control) and was attenuated further with combined inhibition of NO and adenosine (58 ± 9%; P < 0.01 vs. L-NMMA). In protocol 2, percent recovery was reduced with adenosine receptor blockade (74 ± 11% vs. 113 ± 6%, P < 0.01) compared with control drug trials. Percent recovery in FVC was attenuated further with combined inhibition of adenosine and NO (48 ± 11%; P < 0.05 vs. aminophylline). Our data indicate that adenosine contributes to compensatory vasodilation in an NO-independent manner during exercise with acute hypoperfusion.
Figures
Comment in
-
Protection against skeletal muscle hypoperfusion by adenosine and nitric oxide: together alone?J Appl Physiol (1985). 2011 May;110(5):1154-5. doi: 10.1152/japplphysiol.00274.2011. Epub 2011 Mar 10. J Appl Physiol (1985). 2011. PMID: 21393475 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous