

Adaptation of EPEC-EM Curriculum in a Residency with Asynchronous Learning
- PMID: 21293772
- PMCID: PMC3027445
Adaptation of EPEC-EM Curriculum in a Residency with Asynchronous Learning
Abstract
Objective: The Education in Palliative and End-of-life Care for Emergency Medicine Project (EPEC™-EM) is a comprehensive curriculum in palliative and end-of-life care for emergency providers. We assessed the adaptation of this course to an EM residency program using synchronous and asynchronous learning.
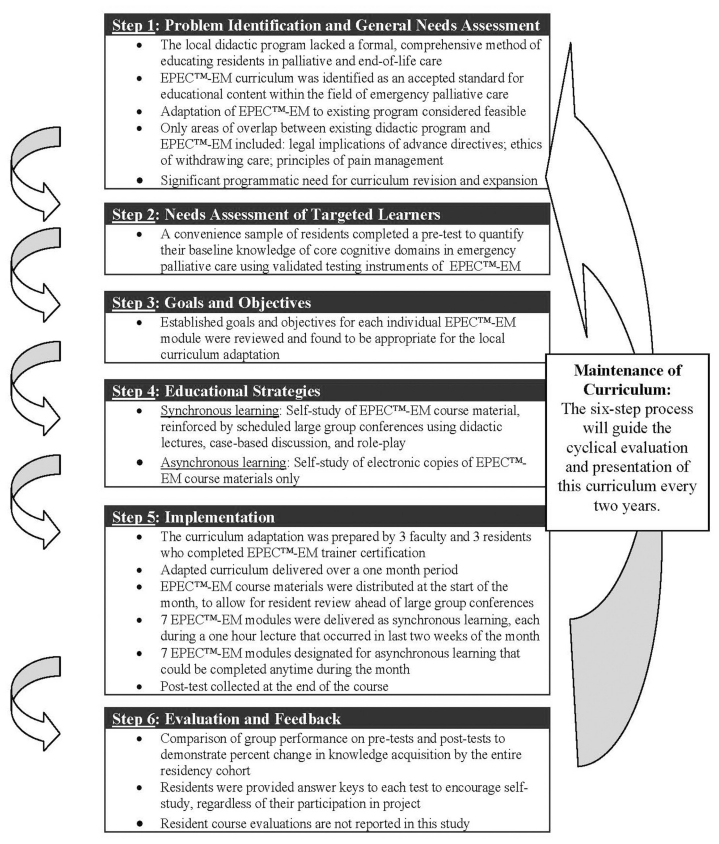
Methods: Curriculum adaptation followed Kern's standardized six-step curriculum design process. Post-graduate year (PGY) 1-4 residents were taught all EPEC™-EM cognitive domains, divided as seven synchronous and seven asynchronous modules. All synchronous modules featured large group didactic lectures and review of EPEC™-EM course materials. Asynchronous modules use only EPEC™-EM electronic course media for resident self-study. Targeted evaluation for EPEC™-EM knowledge objectives was conducted by a prospective case-control crossover study, with synchronous learning serving as the quasi-control, using validated exam tools. We compared de-identified test scores for effectiveness of learning method, using aggregate group performance means for each learning strategy.
Results: Of 45 eligible residents 55% participated in a pre-test for local needs analysis, and 78% completed a post-test to measure teaching method effect. Post-test scores improved across all EPEC™-EM domains, with a mean improvement for synchronous modules of +28% (SD=9) and a mean improvement for asynchronous modules of +30% (SD=18). The aggregate mean difference between learning methods was 1.9% (95% CI -15.3, +19.0). Mean test scores of the residents who completed the post-test were: synchronous modules 77% (SD=12); asynchronous modules 83% (SD=13); all modules 80% (SD=12).
Conclusion: EPEC™-EM adapted materials can improve resident knowledge of palliative medicine domains, as assessed through validated testing of course objectives. Synchronous and asynchronous learning methods appear to result in similar knowledge transfer, feasibly allowing some course content to be effectively delivered outside of large group lectures.
Figures
References
-
- US Department of HHS, CDC. Births, marriages, divorces, and deaths: provisional data for 2007. National Vital Statistics Reports. 2008;56(21):1–3. - PubMed
-
- Ly N, McCaig LF. National hospital ambulatory medical care survey: 2000 outpatient department summary. Adv Data. 2002;(327):1–27. - PubMed
-
- Field MJ, Cassel CK, editors. for Institute of Medicine. Approaching Death: Improving Care at the End of Life. Washington, DC: National Academy Press; 1997. - PubMed
