

An ontology-based nurse call management system (oNCS) with probabilistic priority assessment
- PMID: 21294860
- PMCID: PMC3045288
- DOI: 10.1186/1472-6963-11-26
An ontology-based nurse call management system (oNCS) with probabilistic priority assessment
Abstract
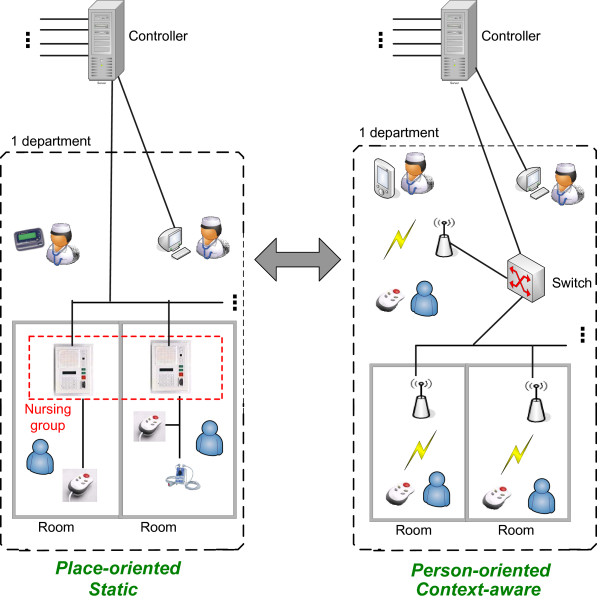
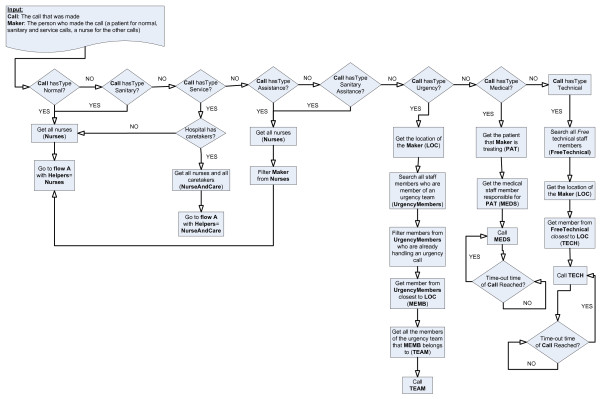
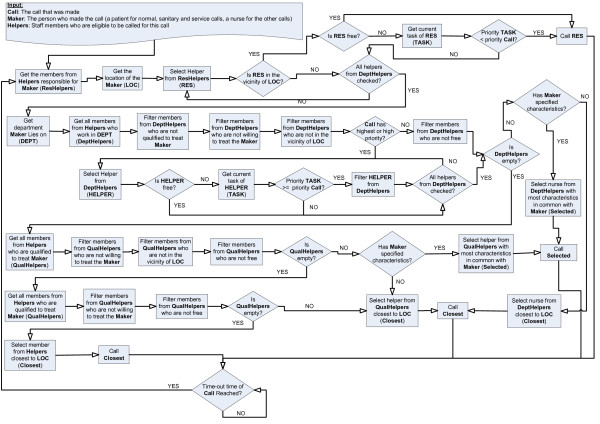
Background: The current, place-oriented nurse call systems are very static. A patient can only make calls with a button which is fixed to a wall of a room. Moreover, the system does not take into account various factors specific to a situation. In the future, there will be an evolution to a mobile button for each patient so that they can walk around freely and still make calls. The system would become person-oriented and the available context information should be taken into account to assign the correct nurse to a call.The aim of this research is (1) the design of a software platform that supports the transition to mobile and wireless nurse call buttons in hospitals and residential care and (2) the design of a sophisticated nurse call algorithm. This algorithm dynamically adapts to the situation at hand by taking the profile information of staff members and patients into account. Additionally, the priority of a call probabilistically depends on the risk factors, assigned to a patient.
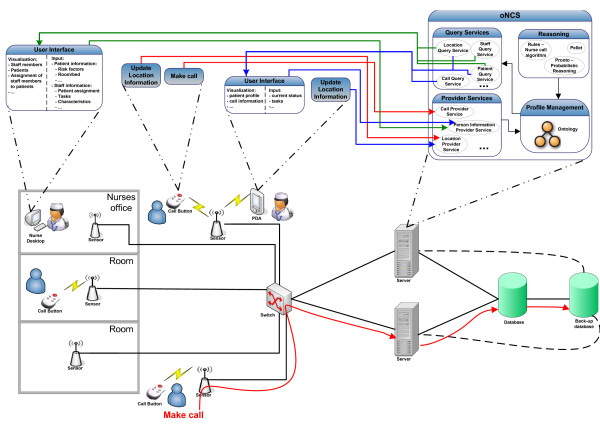
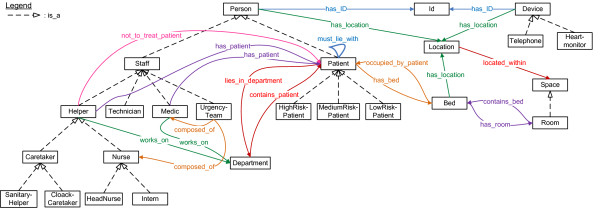
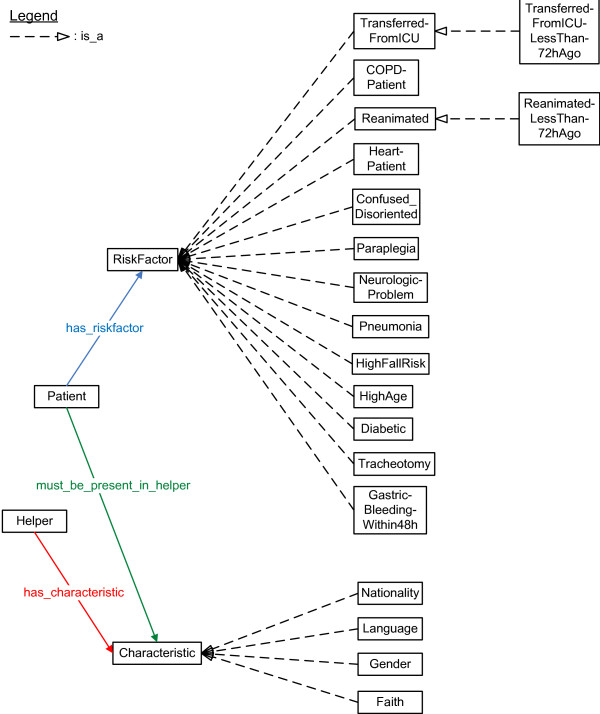
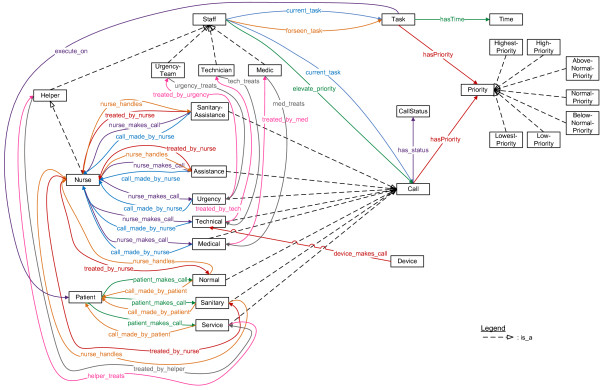
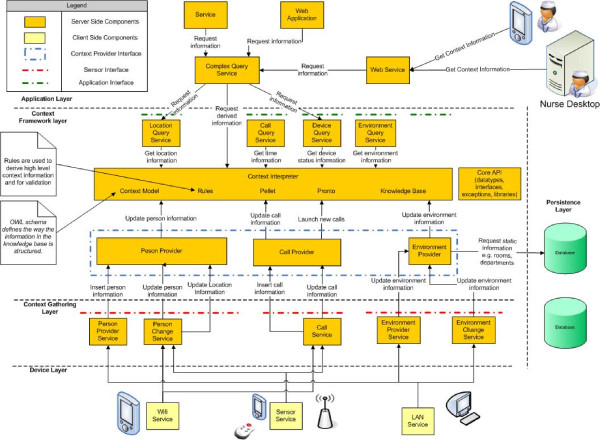
Methods: The ontology-based Nurse Call System (oNCS) was developed as an extension of a Context-Aware Service Platform. An ontology is used to manage the profile information. Rules implement the novel nurse call algorithm that takes all this information into account. Probabilistic reasoning algorithms are designed to determine the priority of a call based on the risk factors of the patient.
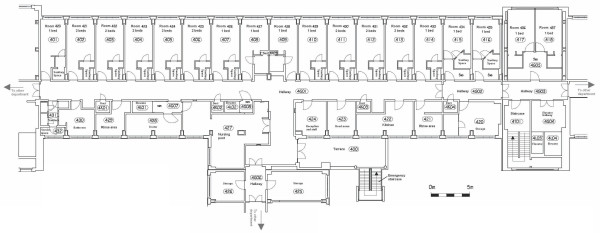
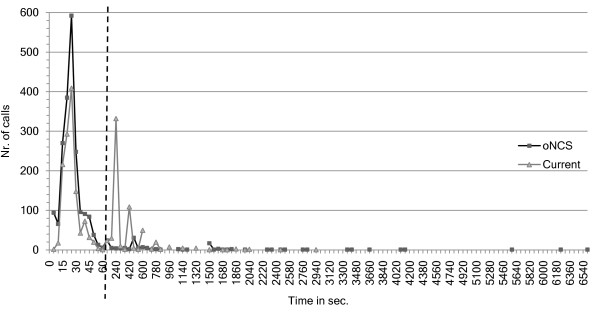
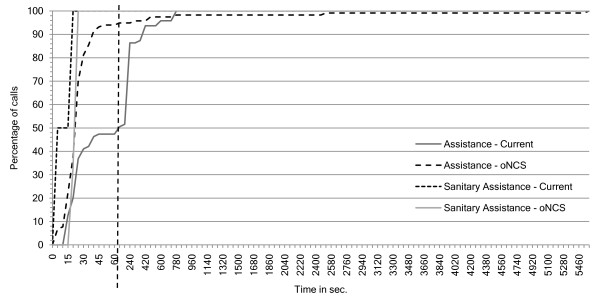
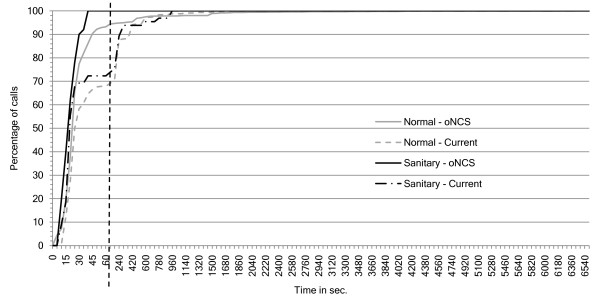
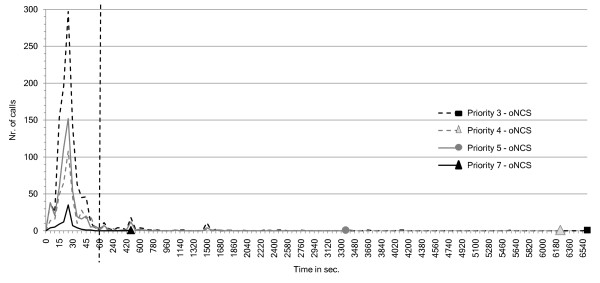
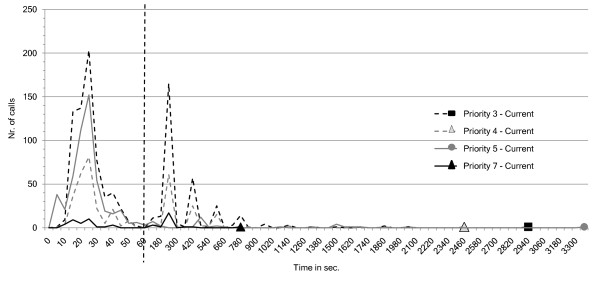
Results: The oNCS system is evaluated through a prototype implementation and simulations, based on a detailed dataset obtained from Ghent University Hospital. The arrival times of nurses at the location of a call, the workload distribution of calls amongst nurses and the assignment of priorities to calls are compared for the oNCS system and the current, place-oriented nurse call system. Additionally, the performance of the system is discussed.
Conclusions: The execution time of the nurse call algorithm is on average 50.333 ms. Moreover, the oNCS system significantly improves the assignment of nurses to calls. Calls generally have a nurse present faster and the workload-distribution amongst the nurses improves.
Figures
References
-
- Van Hoecke S, Decruyenaere J, Danneels C, Taveirne K, Colpaert K, Hoste E, Dhoedt B, De Turck F. Service-oriented subscription management of medical decision data in the intensive care unit. Methods of Information in Medicine. 2008;47(4):364–380. - PubMed
-
- Colpaert K, Van Belleghem S, Benoit D, Steurbaut K, Van Hoecke S, De Turck F, Decruyenaere J. Has information technology finally been adopted in intensive care units? Proceedings of the 22nd Annual Congress of the European Society of Intensive Care Medicine: Oct 11-14 2009; Vienna, Austria. 2009. p. 235.
-
- Tentori M, Segura D, Favela J. Mobile Health Solutions for Biomedical Applications. New York: Medical Information Science Reference; 2009. Monitoring Hospital Patients Using Ambient Displays; pp. 143–158.
-
- Wachter GW. Hospitals Unplugged: The Wireless Revolution Reaches Healthcare. Telemedicine Information Exchange. 2001.
-
- Miller ET, Deets C, Miller R. Nurse call and the work environment: lessons learned. J Nurs Care Qual. 2000;15(3):7–15.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
