

Adjuvant radiation therapy in metastatic lymph nodes from melanoma
- PMID: 21294913
- PMCID: PMC3041681
- DOI: 10.1186/1748-717X-6-12
Adjuvant radiation therapy in metastatic lymph nodes from melanoma
Abstract
Purpose: To analyze the outcome after adjuvant radiation therapy with standard fractionation regimen in metastatic lymph nodes (LN) from cutaneous melanoma.
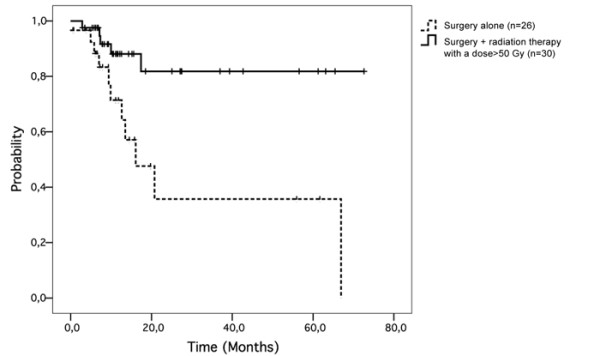
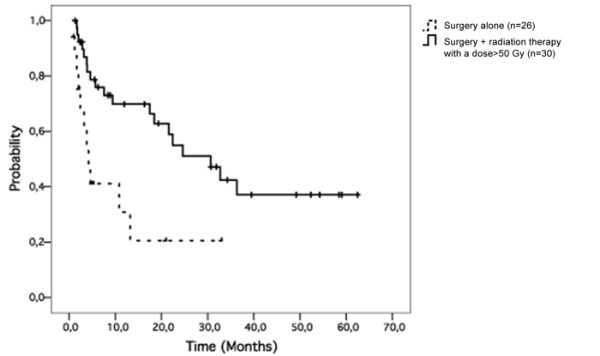
Patients and methods: 86 successive patients (57 men) were treated for locally advanced melanoma in our institution. 60 patients (69%) underwent LN dissection followed by radiation therapy (RT), while 26 patients (31%) had no radiotherapy.
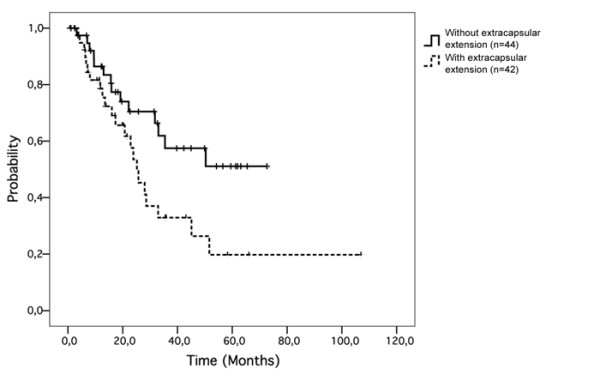
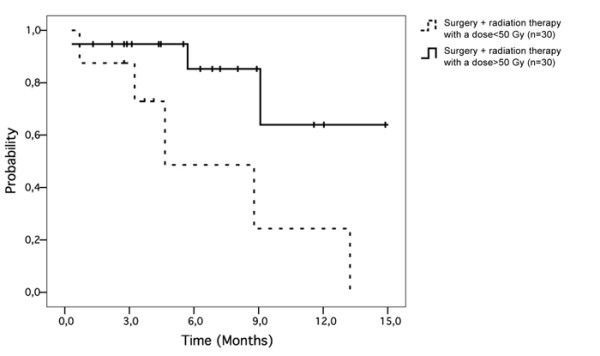
Results: The median number of resected LN was 12 (1 to 36) with 2 metastases (1 to 28). Median survival after the first relapse was 31.8 months. Extracapsular extension was a significant prognostic factor for regional control (p = 0.019). Median total dose was 50 Gy (30 to 70 Gy). A standard fractionation regimen was used (2 Gy/fraction). Median number of fractions was 25 (10 to 44 fractions). Patients were treated with five fractions/week. Patients with extracapsular extension treated with surgery followed by RT (total dose ≥50 Gy) had a better regional control than patients treated by surgery followed by RT with a total dose <50 Gy (80% vs. 35% at 5-year follow-up; p = 0.004).
Conclusion: Adjuvant radiotherapy was able to increase regional control in targeted sub-population (LN with extracapsular extension).
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
