

Trends in comorbidity, disability, and polypharmacy in heart failure
- PMID: 21295193
- PMCID: PMC3237399
- DOI: 10.1016/j.amjmed.2010.08.017
Trends in comorbidity, disability, and polypharmacy in heart failure
Abstract
Background: Comorbidity, disability, and polypharmacy commonly complicate the care of patients with heart failure. These factors can change biological response to therapy, reduce patient ability to adhere to recommendations, and alter patient preference for treatment and outcome. Yet, a comprehensive understanding of the complexity of patients with heart failure is lacking. Our objective was to assess trends in demographics, comorbidity, physical function, and medication use in a nationally representative, community-based heart failure population.
Methods: Using data from the National Health and Nutrition Examination Survey, we analyzed trends across 3 survey periods (1988-1994, 1999-2002, 2003-2008).
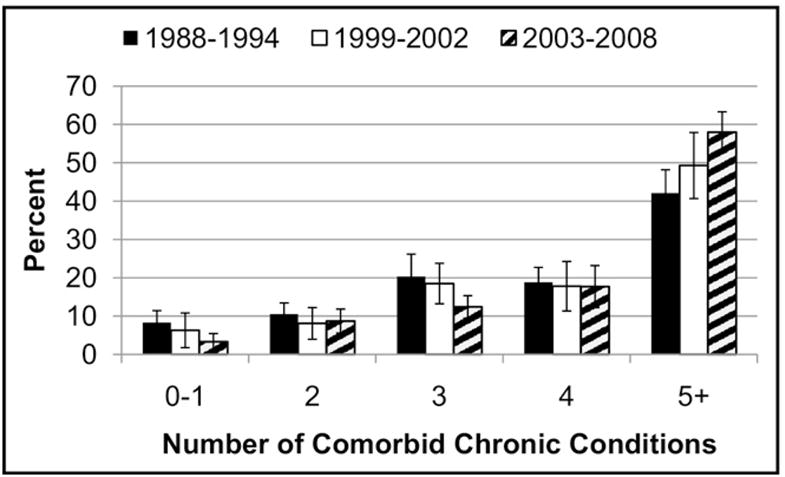
Results: We identified 1395 participants with self-reported heart failure (n=581 in 1988-1994, n=280 in 1999-2002, n=534 in 2003-2008). The proportion of patients with heart failure who were ≥80 years old increased from 13.3% in 1988-1994 to 22.4% in 2003-2008 (P <.01). The proportion of patients with heart failure who had 5 or more comorbid chronic conditions increased from 42.1% to 58.0% (P <.01). The mean number of prescription medications increased from 4.1 to 6.4 prescriptions (P <.01). The prevalence of disability did not increase but was substantial across all years.
Conclusion: The phenotype of patients with heart failure changed substantially over the last 2 decades. Most notably, more recent patients have a higher percentage of very old individuals, and the number of comorbidities and medications increased markedly. Functional disability is prevalent, although it has not changed. These changes suggest a need for new research and practice strategies that accommodate the increasing complexity of this population.
Copyright © 2011 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Tinetti ME, Bogardus ST, Jr, Agostini JV. Potential pitfalls of disease-specific guidelines for patients with multiple conditions. N Engl J Med. 2004;351(27):2870–2874. - PubMed
-
- Boyd CM, Darer J, Boult C, et al. Clinical practice guidelines and quality of care for older patients with multiple comorbid diseases: implications for pay for performance. JAMA. 2005;294(6):716–724. - PubMed
-
- O’Connor PJ. Adding value to evidence-based clinical guidelines. JAMA. 2005;294(6):741–743. - PubMed
-
- Levy D, Kenchaiah S, Larson MG, et al. Long-term trends in the incidence of and survival with heart failure. N Engl J Med. 2002;347(18):1397–1402. - PubMed
-
- Roger VL, Weston SA, Redfield MM, et al. Trends in heart failure incidence and survival in a community-based population. JAMA. 2004;292(3):344–350. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
