

MR diffusion tensor and perfusion-weighted imaging in preoperative grading of supratentorial nonenhancing gliomas
- PMID: 21297125
- PMCID: PMC3064693
- DOI: 10.1093/neuonc/noq197
MR diffusion tensor and perfusion-weighted imaging in preoperative grading of supratentorial nonenhancing gliomas
Abstract
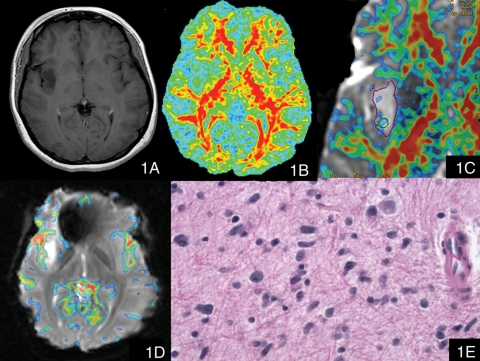
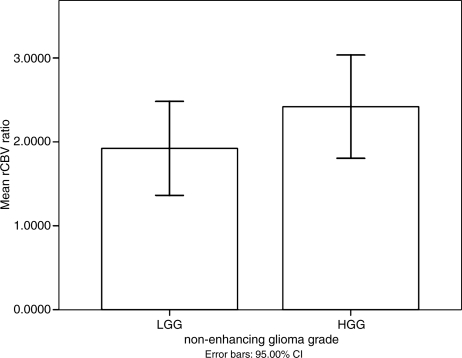
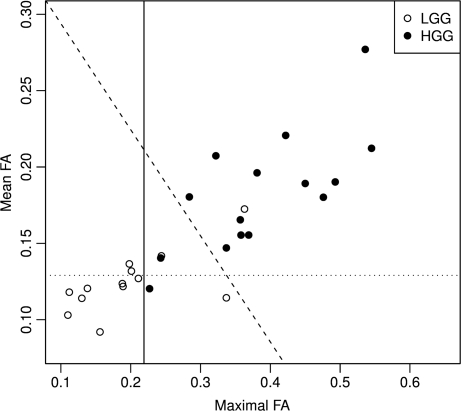
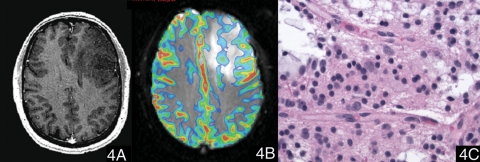
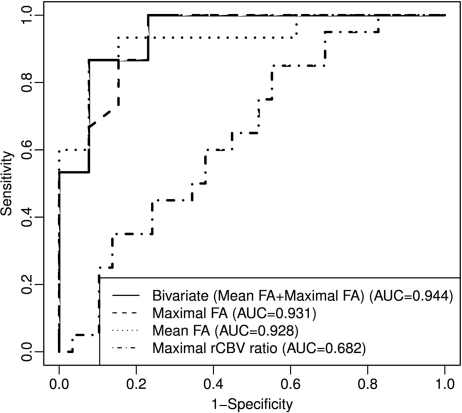
We evaluate the value of MR diffusion tensor imaging (DTI) and dynamic susceptibility-weighted contrast material-enhanced perfusion-weighted imaging (PWI) in preoperative grading of supratentorial nonenhancing gliomas. This institutional review board-approved, Health Insurance Portability and Accountability Act-compliant retrospective study involved 52 patients: 37 with low-grade gliomas (LGGs) and 15 with high-grade gliomas (HGGs). The mean trace apparent diffusion coefficient (ADC), minimal ADC, mean fractional anisotropy (FA), maximal FA, and maximal relative cerebral blood volume (rCBV) ratio of the lesions were measured and compared between LGG and HGG. The efficacy of the above parameters in grading supratentorial nonenhancing gliomas was evaluated. There was no significant difference in rCBV ratio, minimal ADC, and mean ADC between LGG and HGG (p > 0.05). The mean and maximal FA values of LGG were significantly lower than the values of HGG (p < 0.001). The receiver operating characteristic analysis showed that the mean FA with a cutoff value of 0.129 and the maximal FA with a cutoff value of 0.219 could differentiate between LGG and HGG with specificity of 69.2% and 76.9%, respectively, and sensitivity of 93.3% and 100.0%, respectively. The combination of mean FA and maximal FA based on the linear discriminant analysis improved the diagnostic accuracy with specificity of 92.3% and sensitivity of 86.7%. These findings were better than maximal rCBV ratio, mean ADC, and minimum ADC. The mean FA and maximal FA, used individually or combined, may be useful in preoperative grading of supratentorial nonenhancing gliomas.
Figures
References
-
- Ginsberg LE, Fuller GN, Hashmi M, Leeds NE, Schomer DF. The significance of lack of MR contrast enhancement of supratentorial brain tumors in adults: Histopathological evaluation of a series. Surg Neurol. 1998;49:436–440. - PubMed
-
- Fan GG, Deng QL, Wu ZH, Guo QY. Usefulness of diffusion/perfusion-weighted MRI in patients with non-enhancing supratentorial brain gliomas: A valuable tool to predict tumour grading? Br J Radiol. 2006;79:652–658. - PubMed
-
- Mihara F, Numaguchi Y, Rothman M, Kristt D, Fiandaca M, Swallow L. Non-enhancing supratentorial malignant astrocytomas: MR features and possible mechanisms. Radiat Med. 1995;13:11–17. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
