

Is there a difference in clinical outcomes, inflammation, and hypermetabolism between scald and flame burn?
- PMID: 21297515
- PMCID: PMC3672859
- DOI: 10.1097/PCC.0b013e31820ac2c5
Is there a difference in clinical outcomes, inflammation, and hypermetabolism between scald and flame burn?
Abstract
Objective: Severe thermal injury induces inflammatory and hypermetabolic responses that are associated with morbidity and mortality. However, it is not well-documented whether the causes of burns affect inflammation, hypermetabolism, and morbidity. The aim of the present study was to determine whether there is a difference in degree of inflammation, hypermetabolism, endocrine and acute-phase response, and clinical outcome between pediatric patients with scald and flame burns.
Interventions: None.
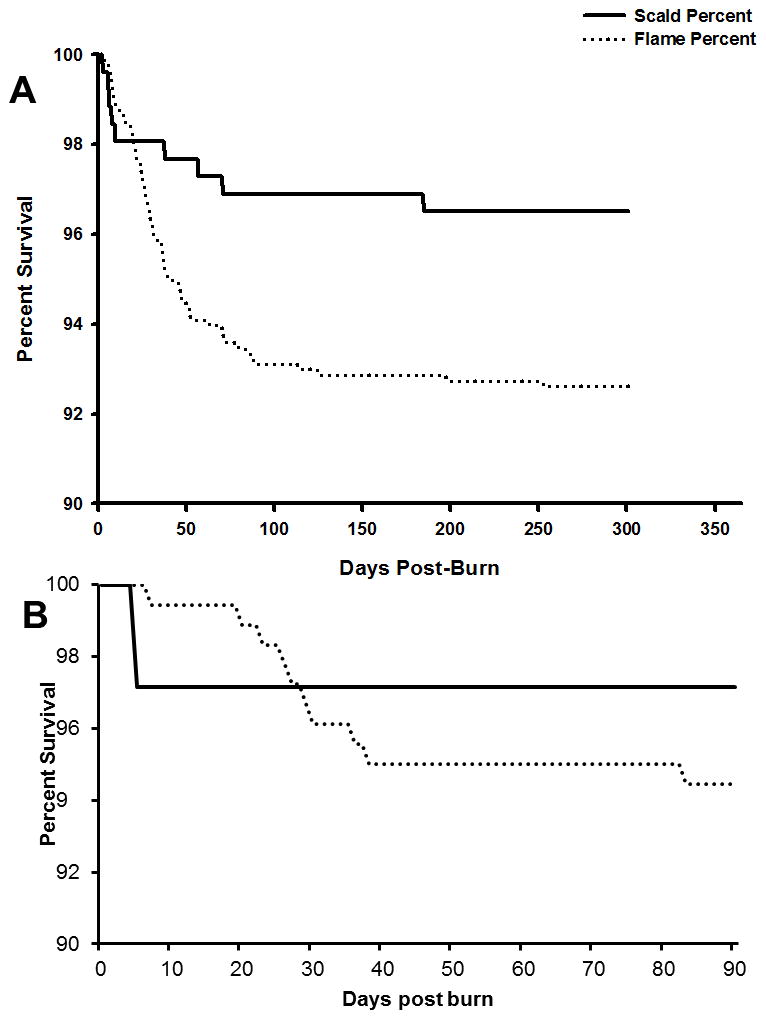
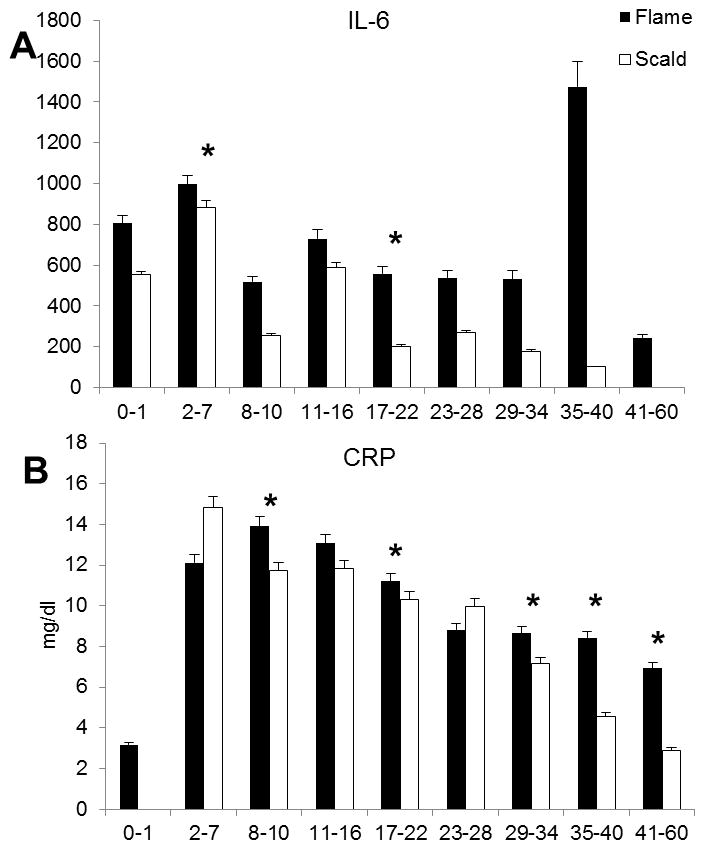
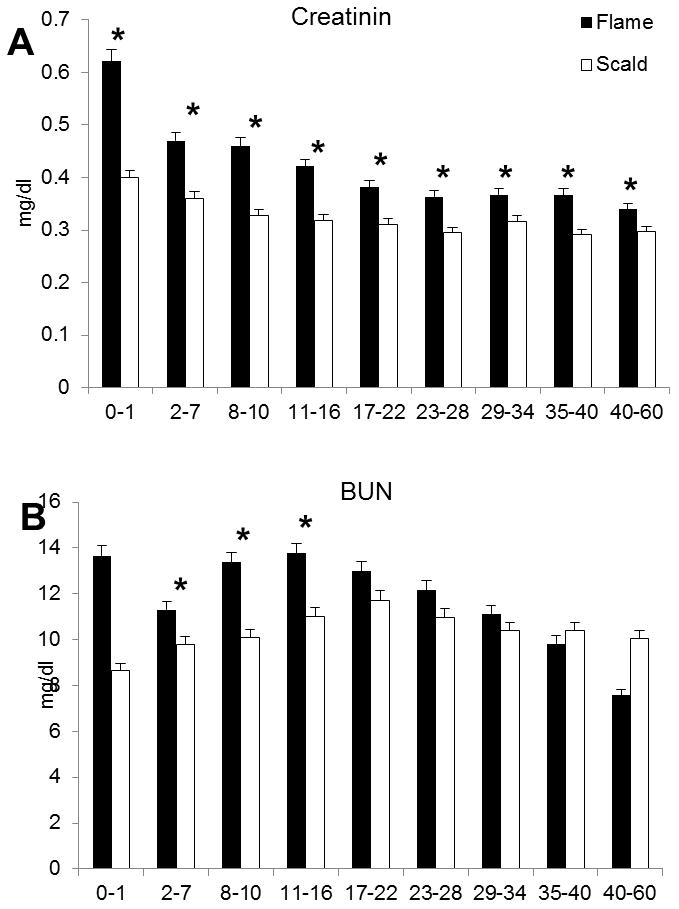
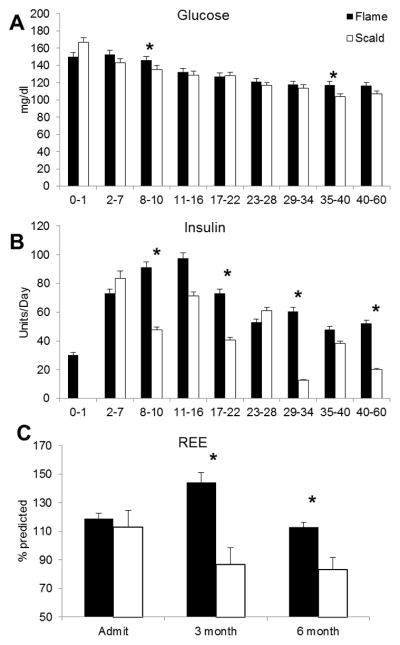
Measurements and main results: Children with burns requiring surgical intervention were enrolled in this cohort study and divided into two groups, scald or flame burn. In a second assignment, we analyzed the study populations in representative subgroups containing individuals with third-degree burns of 40% to 60% total body surface area. We determined clinical outcomes, resting energy expenditures, cytokine profiles, acute-phase proteins, constitutive proteins, and hormone panels. Statistical analysis was evaluated by analysis of variance, Student's t test corrected with the Bonferroni post hoc test, and the propensity score. Statistical significance was set at p < .05. A total of 912 patients were identified. Six hundred seventy-four had a flame burn and 238 had a scald burn. There was a significant difference (p < .05) in burn size (flame, 48% ± 23%; scald, 40% ± 21%), third-degree burn (flame, 39% ± 27%; scald 22% ± 25%), age (flame, 8 ± 5 yrs; scald, 3 ± 3 yrs), and mortality between groups. Propensity analysis confirmed the type of burn as a significant risk factor for morbidity and mortality. Subanalysis conducted in a representative patient group suffering from 40% to 60% burn total body surface area revealed that flame burns lead to significantly increased hypermetabolic, inflammatory, and acute-phase responses when compared to scald burns (p < .05). The frequency of sepsis was 3% in the scald burn group, while it was 14% in the flame group (p < .001). Multiorgan failure occurred in 14% of the scald patients, while it occurred in 17% of flame patients. The mortality in patients suffering from a scald burn was 3% compared to 6% in the flame-burned group (p < .05).
Conclusion: The type of burn affects hypermetabolism, inflammation, acute-phase responses, and mortality postburn.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
The treatment effect of operative intervention for flame versus scald burns in resource-limited settings.Burns. 2024 Dec;50(9):107248. doi: 10.1016/j.burns.2024.08.014. Epub 2024 Aug 18. Burns. 2024. PMID: 39447288
-
The effect of burn mechanism on pediatric mortality in Malawi: A propensity weighted analysis.Burns. 2021 Feb;47(1):222-227. doi: 10.1016/j.burns.2019.12.018. Epub 2020 Dec 1. Burns. 2021. PMID: 33277092 Free PMC article.
-
Burn size determines the inflammatory and hypermetabolic response.Crit Care. 2007;11(4):R90. doi: 10.1186/cc6102. Crit Care. 2007. PMID: 17716366 Free PMC article.
-
The Epidemiology of Burn Injuries in Saudi Arabia: A Systematic Review.J Burn Care Res. 2020 Sep 23;41(5):1122-1127. doi: 10.1093/jbcr/iraa084. J Burn Care Res. 2020. PMID: 32479634
-
The role of the musculoskeletal system in post-burn hypermetabolism.Metabolism. 2019 Aug;97:81-86. doi: 10.1016/j.metabol.2019.06.001. Epub 2019 Jun 8. Metabolism. 2019. PMID: 31181216 Free PMC article. Review.
Cited by
-
Assessment of Prehospital Care for Pediatric Patients with Thermal Injuries: A Retrospective Study.J Clin Med. 2025 Jun 9;14(12):4063. doi: 10.3390/jcm14124063. J Clin Med. 2025. PMID: 40565809 Free PMC article.
-
The treatment effect of operative intervention for flame versus scald burns in resource-limited settings.Burns. 2024 Dec;50(9):107248. doi: 10.1016/j.burns.2024.08.014. Epub 2024 Aug 18. Burns. 2024. PMID: 39447288
-
Development and Validation of Indicators for Population Injury Surveillance in Hong Kong: Development and Usability Study.JMIR Public Health Surveill. 2022 Aug 18;8(8):e36861. doi: 10.2196/36861. JMIR Public Health Surveill. 2022. PMID: 35980728 Free PMC article. Review.
-
Burn Induces Browning of the Subcutaneous White Adipose Tissue in Mice and Humans.Cell Rep. 2015 Nov 24;13(8):1538-44. doi: 10.1016/j.celrep.2015.10.028. Epub 2015 Nov 12. Cell Rep. 2015. PMID: 26586436 Free PMC article.
-
Burns in Israel: Etiologic, Demographic, and Clinical trends-A 9-Year Updated Comprehensive Study, 2004-2010 versus 2011-2019.Semin Plast Surg. 2022 Aug 4;36(2):66-74. doi: 10.1055/s-0042-1749094. eCollection 2022 May. Semin Plast Surg. 2022. PMID: 36172009 Free PMC article. Review.
References
-
- Gore DC, Hawkins HK, Chinkes DL, Chung DH, Sanford AP, Herndon DN, Wolf SE. Assessment of adverse events in the demise of pediatric burn patients. J Trauma. 2007;63(4):814–818. - PubMed
-
- Klein MB, Lezotte DL, Fauerbach JA, Herndon DN, Kowalske KJ, Carrougher GJ, deLateur BJ, Holavanahalli R, Esselman PC, San Agustin TB, et al. The National Institute on Disability and Rehabilitation Research burn model system database: a tool for the multicenter study of the outcome of burn injury. J Burn Care Res. 2007;28(1):84–96. - PubMed
-
- Rosenberg M, Robertson C, Murphy KD, Rosenberg L, Mlcak R, Robert RS, Herndon DN, Meyer WJ., 3rd Neuropsychological outcomes of pediatric burn patients who sustained hypoxic episodes. Burns. 2005;31(7):883–889. - PubMed
-
- Murphy KD, Lee JO, Herndon DN. Current pharmacotherapy for the treatment of severe burns. Expert Opin Pharmacother. 2003;4(3):369–384. - PubMed
-
- Thomas S, Wolf SE, Chinkes DL, Herndon DN. Recovery from the hepatic acute phase response in the severely burned and the effects of long-term growth hormone treatment. Burns. 2004;30(7):675–679. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
