

Efficacy and outcomes of dynamic-plated single-level anterior diskectomy/fusion with additional analysis of comparative costs
- PMID: 21297931
- PMCID: PMC3031047
- DOI: 10.4103/2152-7806.76146
Efficacy and outcomes of dynamic-plated single-level anterior diskectomy/fusion with additional analysis of comparative costs
Abstract
Background: Few studies focus on the fusion rates and outcomes for single-level anterior cervical diskectomy/fusion (1-ACDF) utilizing iliac autograft and dynamic plates.
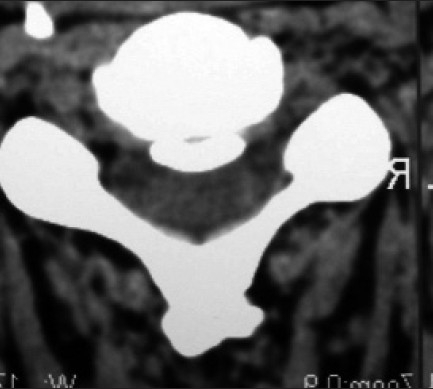
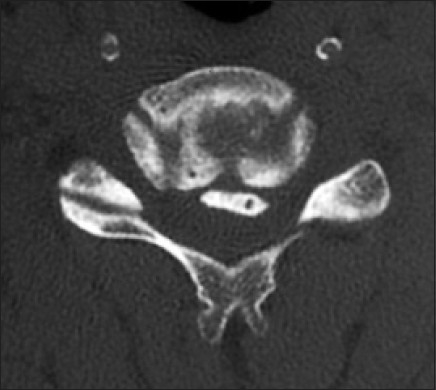
Methods: Fusion rates and outcomes were prospectively evaluated in 60 consecutive patients undergoing 1-ACDF utilizing iliac autograft and dynamic plates (ABC; Aesculap, Tuttlingen, Germany). Eighteen patients had radiculopathy, while 42 were myelopathic (average Nurick Score 3.3). Pathology included single-level disc disease/spondylosis (38 patients) and/or ossification of the posterior longitudinal ligament (OPLL, 22 patients). Fusion was assessed at 3, 6, and up to 12 months postoperatively utilizing dynamic X-rays and 2D-CT scans. Outcomes were evaluated up to 24 months postoperatively utilizing Odom's Criteria, Nurick Grades, and Short-Form 36 (SF-36) outcome questionnaires. Patients were followed for an average of 4.8 postoperative years (minimum 2 years).
Results: Although dynamic X-rays/2D-CT studies documented 100% fusion an average of 3.8 months (range 2.5-8 months] postoperatively, 5 heavy smokers exhibited delayed fusions [6-8 months postoperatively]. Two years postoperatively, the average Nurick Score was 0.3 (mild radiculopathy), while Odom's Criteria revealed 52 excellent, 6 good, and 2 fair outcomes [the latter 8 patients were heavy smokers]). Utilizing SF-36 outcome questionnaires, patients markedly improved (>10.0 point gain) on 5 of 8 Health Scales within 6 months, 7 of 8 within 1 year, and all 8 within 2 postoperative years.
Conclusions: For 60 patients undergoing 1-ACDF utilizing dynamic plates, ultimately a 100% fusion rate was achieved (5 heavy smokers exhibited delayed fusions). Two years postoperatively, Nurick Grades, Odom's Criteria, and SF-36 questionnaires revealed adequate outcomes.
Keywords: Anterior Cervical Diskectomy/Fusion; Autograft; Dynamic Plates; Fusion Rates; SF-36 Outcomes; Single-level.
Figures



References
-
- Balabhadra R, Kim DH, Zhang HY. Anterior cervical fusion using dense cancellous allografts and dynamic plating. Neurosurgery. 2004;54:1405–11. - PubMed
-
- Buttermann GR. Prospective nonrandomized comparison of an allograft with bone morphogenetic protein versus an iliac-crest autograft in anterior cervical diskectomy and fusion. Spine J. 2008;8:426–35. - PubMed
-
- Castro FP, Jr, Holt RT, Maid M, Whitecloud TS., 3rd A cost analysis of two anterior cervical fusion procedures. J Spinal Disord. 2000;13:511–4. - PubMed
-
- Epstein NE, Schwall GS, Reilley T, Insinna T, Bahnken A, Hood DC. Surgeon choices, and the choice of surgeons, affect total hospital charges for single-level anterior cervical surgery. Spine. 2010 [in press] - PubMed
LinkOut - more resources
Full Text Sources
