

Increased rate of CD4+ T-cell decline and faster time to antiretroviral therapy in HIV-1 subtype CRF01_AE infected seroconverters in Singapore
- PMID: 21298051
- PMCID: PMC3029292
- DOI: 10.1371/journal.pone.0015738
Increased rate of CD4+ T-cell decline and faster time to antiretroviral therapy in HIV-1 subtype CRF01_AE infected seroconverters in Singapore
Abstract
Background: It remains controversial as to whether HIV-1 subtypes influence disease progression. Singapore offers a unique opportunity to address this issue due to the presence of co-circulating subtypes. We compared subtype CRF01_AE and non-CRF01_AE infected patients, with regards to estimated annual rate of CD4+ T-cell loss and time from estimated data of seroconversion (EDS) to antiretroviral therapy (ART).
Methods: We recruited ART-naive patients with known dates of seroconversion between October 2002 and December 2007 at the Singapore Communicable Disease Centre, the national reference treatment centre. Multilevel mixed-effects models were used to analyse the rate of CD4+ T-cell decline. Time from EDS to ART was analyzed with the Kaplan-Meier survival method and compared with Cox proportional hazards models.
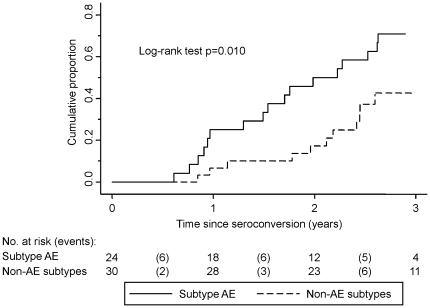
Results: 54 patients with previously assigned HIV-1 subtypes (24 CRF01_AE, 17 B, 8 B', 1 CRF33_01B, 3 CRF34_01B and 1 G) were observed for 89 patient-years. Subtype CRF01_AE and non-CRF01_AE infected patients did not differ in age, gender, risk factor, rate of symptomatic seroconversion, baseline CD4+ T-cell count, log(10) viral load or haemoglobin concentration. The estimated annual rate of CD4+ T-cell loss was 58 cells/mm(3)/year (95% CI: 7 to 109; P = 0.027) greater in subtype CRF01_AE infected patients compared to non-CRF01_AE patients, after adjusting for age, baseline CD4+ T-cell count and baseline log(10) viral load. The median time from EDS to ART was 1.8 years faster comparing CRF01_AE to non-CRF01_AE infected patient with a 2.5 times (95% CI: 1.2-5.0; P = 0.013) higher hazard for ART initiation, after controlling for age, baseline CD4+ T-cell count and baseline log(10) viral load.
Conclusions: Infecting subtype significantly impacted the rate of CD4+ T-cell loss and time to treatment in this cohort. Studies to understand the biological basis for this difference could further our understanding of HIV pathogenesis.
Conflict of interest statement
Figures
Similar articles
-
After 18 months of antiretroviral therapy, total HIV DNA decreases more pronouncedly in patients infected by CRF01_AE than in those infected by subtype B and CRF07_BC.Microbiol Immunol. 2018 Apr;62(4):248-254. doi: 10.1111/1348-0421.12578. Epub 2018 Mar 26. Microbiol Immunol. 2018. PMID: 29377267
-
Low CD4 count was characterized in recent HIV CRF01_AE infection and it rapidly increased to reach a peak in the first year since ART initiation.BMC Infect Dis. 2025 Mar 31;25(1):443. doi: 10.1186/s12879-025-10799-5. BMC Infect Dis. 2025. PMID: 40165131 Free PMC article.
-
HIV-1 CRF01_AE subtype and HIV-1 DNA level among patients with chronic HIV-1 infection: a correlation study.BMC Infect Dis. 2020 Jan 21;20(1):66. doi: 10.1186/s12879-020-4785-6. BMC Infect Dis. 2020. PMID: 31964364 Free PMC article. Clinical Trial.
-
Evidence that HIV-1 CRF01_AE is associated with low CD4+T cell count and CXCR4 co-receptor usage in recently infected young men who have sex with men (MSM) in Shanghai, China.PLoS One. 2014 Feb 21;9(2):e89462. doi: 10.1371/journal.pone.0089462. eCollection 2014. PLoS One. 2014. PMID: 24586795 Free PMC article.
-
Pathogenesis of infections in HIV-infected individuals: insights from primary immunodeficiencies.Curr Opin Immunol. 2017 Oct;48:122-133. doi: 10.1016/j.coi.2017.09.002. Epub 2017 Oct 6. Curr Opin Immunol. 2017. PMID: 28992464 Free PMC article. Review.
Cited by
-
The Molecular Epidemiological and Immunological Characteristics of HIV-1 CRF01_AE/B Recombinants in Nanjing, China.Front Microbiol. 2022 Jul 15;13:936502. doi: 10.3389/fmicb.2022.936502. eCollection 2022. Front Microbiol. 2022. PMID: 35910646 Free PMC article.
-
Immune reconstruction effectiveness of combination antiretroviral therapy for HIV-1 CRF01_AE cluster 1 and 2 infected individuals.Emerg Microbes Infect. 2022 Dec;11(1):158-167. doi: 10.1080/22221751.2021.2017755. Emerg Microbes Infect. 2022. PMID: 34895083 Free PMC article.
-
HIV-1 subtype CRF01_AE and B differ in utilization of low levels of CCR5, Maraviroc susceptibility and potential N-glycosylation sites.Virology. 2017 Dec;512:222-233. doi: 10.1016/j.virol.2017.09.026. Epub 2017 Oct 9. Virology. 2017. PMID: 29020646 Free PMC article.
-
HIV-1 induced bystander apoptosis.Viruses. 2012 Nov 9;4(11):3020-43. doi: 10.3390/v4113020. Viruses. 2012. PMID: 23202514 Free PMC article. Review.
-
Critical amino acid residues and potential N-linked glycosylation sites contribute to circulating recombinant form 01_AE pathogenesis in Northeast China.AIDS. 2019 Jul 15;33(9):1431-1439. doi: 10.1097/QAD.0000000000002197. AIDS. 2019. PMID: 30889014 Free PMC article.
References
-
- Joint United Nations Program on HIV/AIDS (UNAIDS) WHOW. UNAIDS; 2007. AIDS Epidemic Update: November 2009.
-
- Kaleebu P, French N, Mahe C, Yirrell D, Watera C, et al. Effect of human immunodeficiency virus (HIV) type 1 envelope subtypes A and D on disease progression in a large cohort of HIV-1-positive persons in Uganda. Journal of Infectious Diseases. 2002;185:1244–1250. - PubMed
-
- Keller M, Lu Y, Lalonde RG, Klein MB. Impact of HIV-1 viral subtype on CD4+ T-cell decline and clinical outcomes in antiretroviral naive patients receiving universal healthcare. AIDS. 2009;23:731–737. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
