

Neural mechanisms of angiotensin II-salt hypertension: implications for therapies targeting neural control of the splanchnic circulation
- PMID: 21298369
- PMCID: PMC3076522
- DOI: 10.1007/s11906-011-0188-9
Neural mechanisms of angiotensin II-salt hypertension: implications for therapies targeting neural control of the splanchnic circulation
Abstract
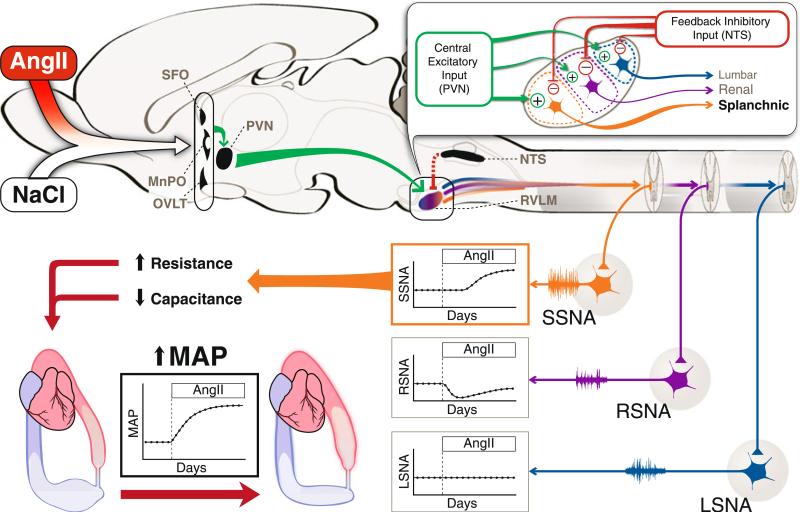
Chronically elevated plasma angiotensin II (AngII) causes a salt-sensitive form of hypertension that is associated with a differential pattern of peripheral sympathetic outflow. This "AngII-salt sympathetic signature" is characterized by a transient reduction in sympathetic nervous system activity (SNA) to the kidneys, no change in SNA to skeletal muscle, and a delayed activation of SNA to the splanchnic circulation. Studies suggest that the augmented sympathetic influence on the splanchnic vascular bed increases vascular resistance and decreases vascular capacitance, leading to hypertension via translocation of blood volume from the venous to the arterial circulation. This unique sympathetic signature is hypothesized to be generated by a balance of central excitatory inputs and differential baroreceptor inhibitory inputs to sympathetic premotor neurons in the rostral ventrolateral medulla. The relevance of these findings to human hypertension and the future development of targeted sympatholytic therapies are discussed.
Figures
References
-
- Chobanian AV. The hypertension paradox—More uncontrolled disease despite improved therapy. N Engl J Med. 2009;361:878–97. - PubMed
-
- Symplicity HTN-2 Investigators: Renal sympathetic denervation in patients with treatment-resistant hypertension (The Symplicity HTN-2 Trial): a randomised controlled trial. Lancet. 2010;376:1903–1909. [This study demonstrated long-lasting decreases in arterial pressure in patients with drug-resistant hypertension following bilateral renal denervation by radiofrequency ablation. This new technology suggests that regional sympathetic ablation may be a new direction for the development of devices to treat hypertension.] - PubMed
-
- Smithwick RH. Splanchnicectomy for essential hypertension; results in 1, 266 cases. JAMA. 1953;152(16):1501–4. - PubMed
-
- Esler M. The sympathetic system and hypertension. Am J Hypertens. 2000;13:995–1055. - PubMed
-
- Esler M, Lambert E, Schlaich MP. Chronic activation of the sympathetic nervous system is the dominant contributor to systemic hypertension. J Appl Physiol. 2010;109(6):1996–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
