

Does speed matter? The impact of operative time on outcome in laparoscopic surgery
- PMID: 21298533
- PMCID: PMC3676304
- DOI: 10.1007/s00464-010-1550-8
Does speed matter? The impact of operative time on outcome in laparoscopic surgery
Abstract
Introduction: Controversy exists concerning the importance of operative time on patient outcomes. It is unclear whether faster is better or haste makes waste or similarly whether slower procedures represent a safe, meticulous approach or inexperienced dawdling. The objective of the present study was to determine the effect of operative time on 30-day outcomes in laparoscopic surgery.
Methods: Patients who underwent laparoscopic general surgery procedures (colectomy, cholecystectomy, Nissen fundoplication, inguinal hernia, and gastric bypass) from the ACS-NSQIP 2005-2008 participant use file were identified. Exclusion criteria were defined a priori to identify same-day admission, elective procedures. Operative time was divided into deciles and summary statistics were analyzed. Univariate analyses using a Cochran-Armitage test for trend were completed. The effect of operative time on 30-day morbidity was further analyzed for each procedure type using multivariate regression controlling for case complexity and additional patient factors. Patients within the highest deciles were excluded to reduce outlier effect.
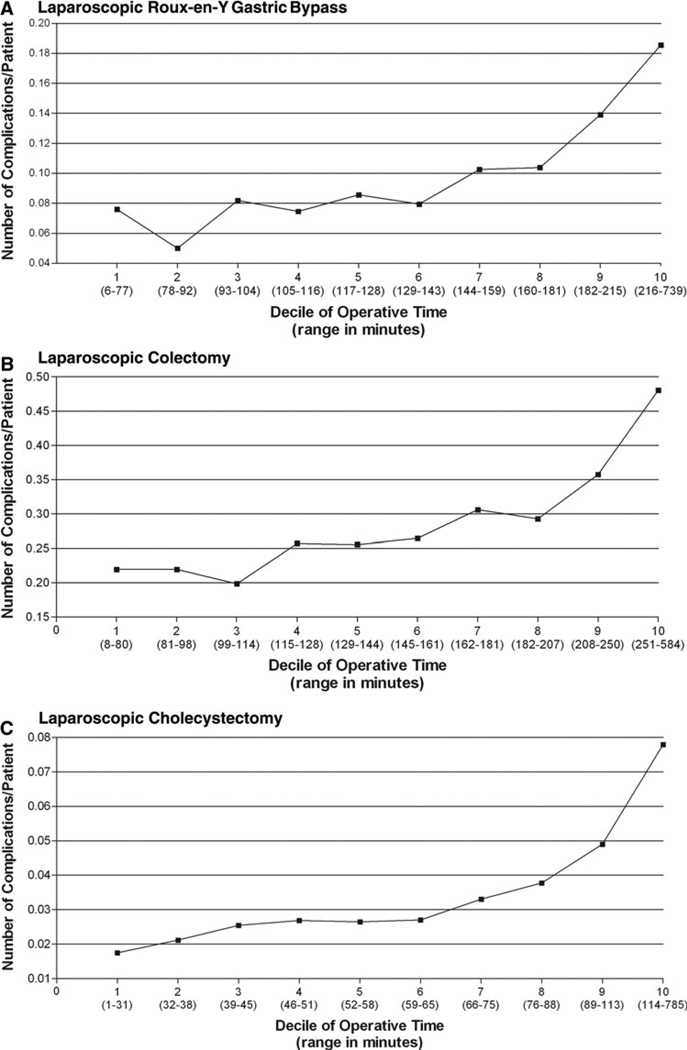
Results: A total of 76,748 elective general surgical patients who underwent laparoscopic procedures were analyzed. Univariate analyses of deciles of operative time demonstrated a statistically significant trend (p<0.0001) toward increasing odds of complications with increasing operative time for laparoscopic colectomy (n=10,135), cholecystectomy (n=37,407), Nissen fundoplication (n=4,934), and gastric bypass (n=17,842). The trend was not found to be significant for laparoscopic inguinal hernia repair (n=6,430; p=0.14). Multivariate modeling revealed the effect of operative time to remain significant after controlling for additional patient factors.
Conclusion: Increasing operative time was associated with increased odds of complications and, therefore, it appears that speed may matter in laparoscopic surgery. These analyses are limited in their inability to adjust for all patient factors, potential confounders, and case complexities. Additional hierarchical multivariate analyses at the surgeon level would be important to examine this relationship further.
Conflict of interest statement
Disclosures Drs. Timothy Jackson, Jeffrey Wannares, R. Todd Lancaster, David Rattner, and Matthew Hutter have no conflicts of interest or financial ties to disclose.
Figures

References
-
- Khuri SF, Henderson WG, Daley J, Jonasson O, Jones RS, Campbell DA, Jr, Fink AS, Mentzer RM, Jr, Steeger JE. The patient safety in surgery study: background, study design, and patient populations. J Am Coll Surg. 2007;204(6):1089–1102. - PubMed
-
- Khuri SF, Daley J, Henderson W, Hur K, Gibbs JO, Barbour G, Demakis J, Irvin G, 3rd, Stremple JF, Grover F, McDonald G, Passaro E, Jr, Fabri PJ, Spencer J, Hammermeister K, Aust JB. Risk adjustment of the postoperative mortality rate for the comparative assessment of the quality of surgical care: results of the National Veterans Affairs Surgical Risk Study. J Am Coll Surg. 1997;185(4):315–327. - PubMed
-
- Daley J, Khuri SF, Henderson W, Hur K, Gibbs JO, Barbour G, Demakis J, Irvin G, III, Stremple JF, Grover F, McDonald G, Passaro E, Jr, Fabri PJ, Spencer J, Hammermeister K, Aust JB, Oprian C. Risk adjustment of the postoperative morbidity rate for the comparative assessment of the quality of surgical care: results of the National Veterans Affairs Surgical Risk Study. J Am Coll Surg. 1997;185(4):328–340. - PubMed
-
- Daley J, Forbes MG, Young GJ, Charns MP, Gibbs JO, Hur K, Henderson W, Khuri SF. Validating risk-adjusted surgical outcomes: site visit assessment of process and structure National VA Surgical Risk Study. J Am Coll Surg. 1997;185(4):341–351. - PubMed
-
- Khuri SF, Henderson WG, Daley J, Jonasson O, Jones RS, Campbell DA, Jr, Fink AS, Mentzer RM, Jr, Neumayer L, Hammermeister K, Mosca C, Healey N. Successful implementation of the Department of Veterans Affairs’ National Surgical Quality Improvement Program in the private sector: the Patient Safety in Surgery study. Ann Surg. 2008;248(2):329–336. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
