

Orofacial airway dimensions in subjects with Class I malocclusion and different growth patterns
- PMID: 21299381
- PMCID: PMC8923554
- DOI: 10.2319/091910-545.1
Orofacial airway dimensions in subjects with Class I malocclusion and different growth patterns
Abstract
Objective: To test the null hypotheses that there are no significant differences in craniofacial structures and orofacial airway dimensions in subjects with Class I malocclusion and different growth patterns.
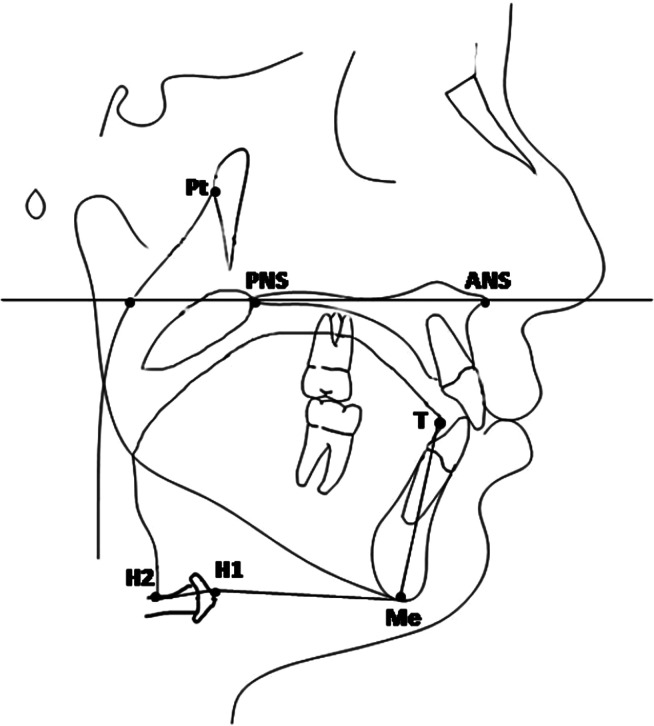
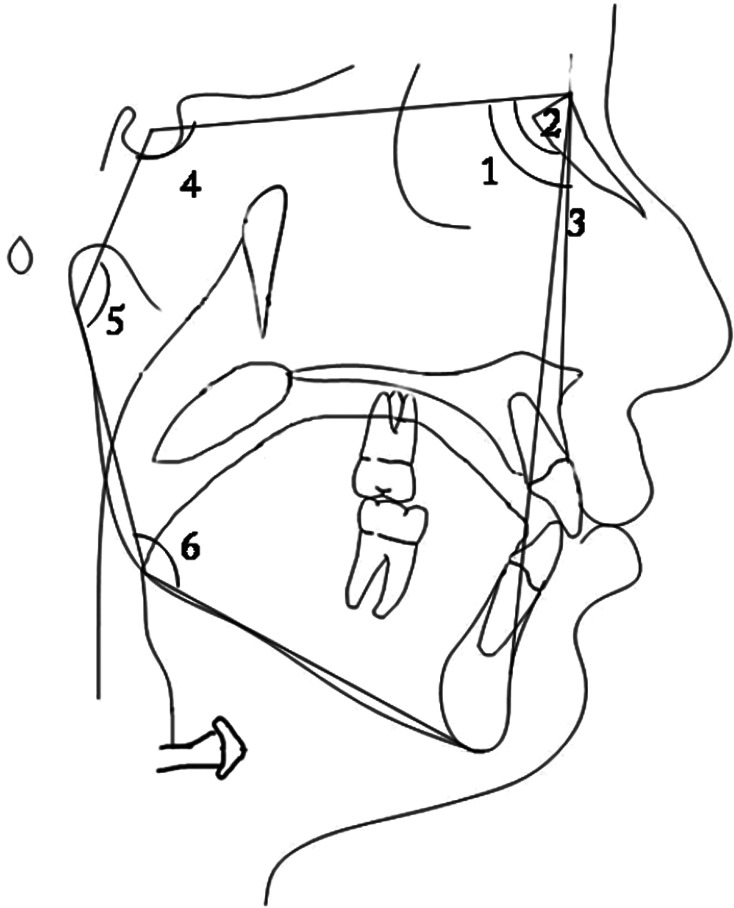
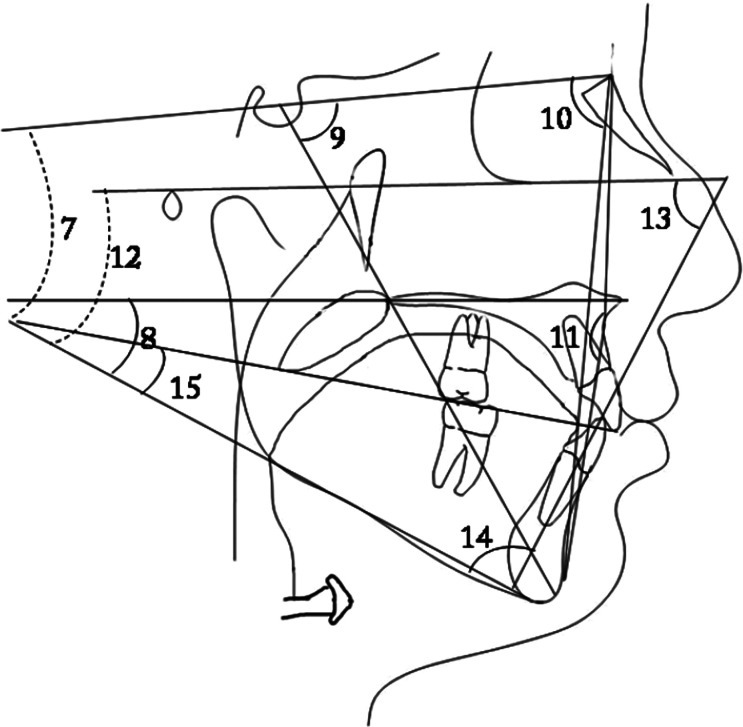
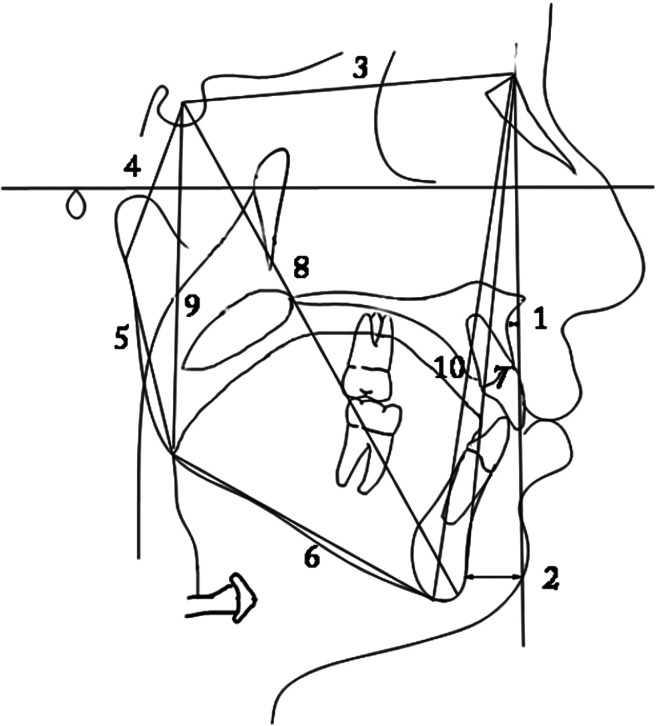
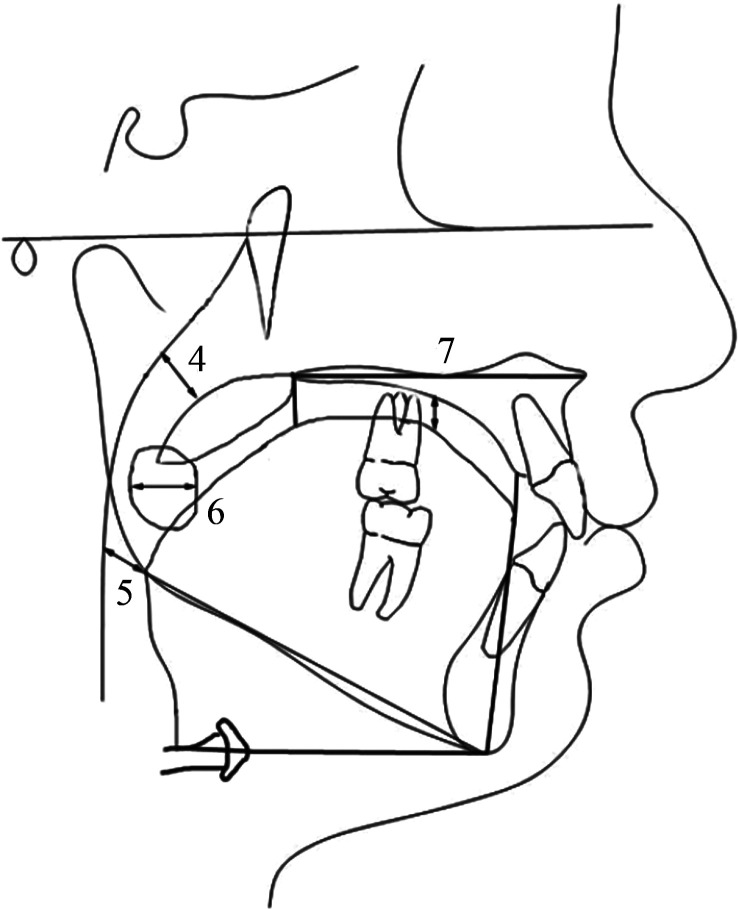
Materials and methods: Lateral cephalometric radiographs of 31 low angle (mean age, 14.0 ± 2.0 years; range, 10.3-16.5 years), 40 high angle (mean age, 12.7 ± 1.6 years; range, 10.1-16.2 years), and 33 normal growth (mean age, 13.9 ± 1.3 years; range, 11.2-16.8 years) subjects with Class I malocclusion were examined. In total, 34 measurements (27 craniofacial and 7 orofacial airways) were evaluated. Groups were constituted according to the SN-MP angle. Group differences were analyzed with analysis of variance (ANOVA) and the Tukey test, at the P < .05 level.
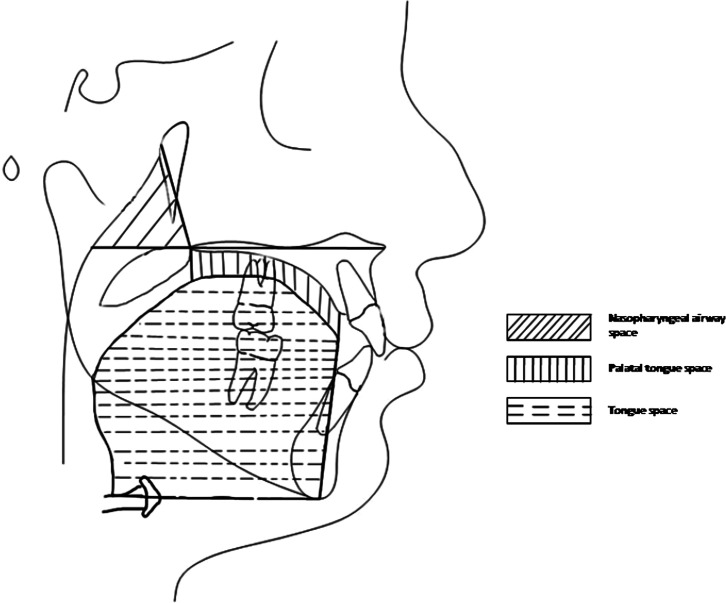
Results: According to ANOVA, only 5 of the 27 craniofacial measurements showed no statistically significant differences among different growth patterns. For orofacial airway measurements, statistically significant differences were found in nasopharyngeal airway space (P < .01), palatal tongue space (P < .05), upper posterior airway space (PAS) (P < .05), and tongue gap (P < .001). No statistically significant orofacial airway differences were determined between low angle and normal growth subjects. High angle subjects had a larger tongue gap than those with normal and low angles (P < .01). Additionally, nasopharyngeal airway space (P < .01) and upper PAS (P < .05) measurements were larger and palatal tongue space (P < .05) was narrower in low angle than in high angle subjects.
Conclusions: The null hypotheses were rejected. Significant differences in craniofacial morphology and orofacial airway dimensions of Class I subjects with different growth patterns were identified.
Figures
References
-
- Nielsen L. Vertical malocclusions: etiology, development, diagnosis and some aspects of treatment. Angle Orthod. 1991;61:247–260. - PubMed
-
- Creekmore T. D. Inhibition or stimulation of the vertical growth of the facial complex, its significance to treatment. Angle Orthod. 1967;37:285–297. - PubMed
-
- Isaacson J. R, Isaacson R. J, Speidel T. M, Worms F. W. Extreme variation in vertical facial growth and associated variation in skeletal and dental relations. Angle Orthod. 1971;41:219–229. - PubMed
-
- Schudy F. F. The rotation of the mandible resulting from growth: its implications in orthodontic treatment. Angle Orthod. 1965;35:36–50. - PubMed
-
- Chung C. H, Mongiovi V. D. Craniofacial growth in untreated skeletal Class I subjects with low, average, and high MP-SN angles: a longitudinal study. Am J Orthod Dentofacial Orthop. 2003;124:670–678. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
