

Randomized trial of zileuton for treatment of COPD exacerbations requiring hospitalization
- PMID: 21299475
- PMCID: PMC3775706
- DOI: 10.3109/15412555.2010.540273
Randomized trial of zileuton for treatment of COPD exacerbations requiring hospitalization
Abstract
Rationale: Leukotrienes have been implicated in the pathogenesis of acute exacerbations of COPD, but leukotriene modifiers have not been studied as a possible therapy for exacerbations.
Objective: We sought to test the safety and efficacy of adding oral zileuton (a 5-lipoxygenase inhibitor) to usual treatment for acute exacerbations of COPD requiring hospitalization.
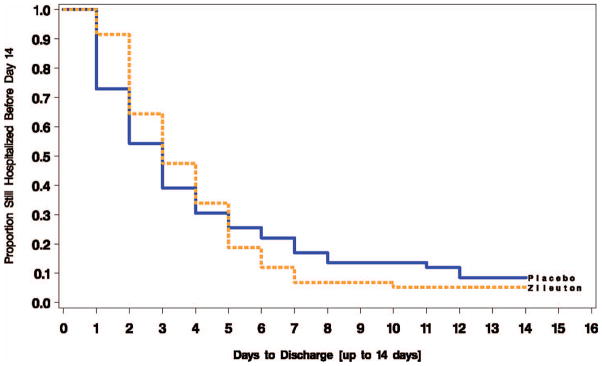
Methods: Randomized double-blind, placebo-controlled, parallel group study of zileuton 600 mg orally, 4 times daily versus placebo for 14 days starting within 12 hours of hospital admission for COPD exacerbation. Primary outcome measure was hospital length of stay; secondary outcomes included treatment failure and biomarkers of leukotriene production.
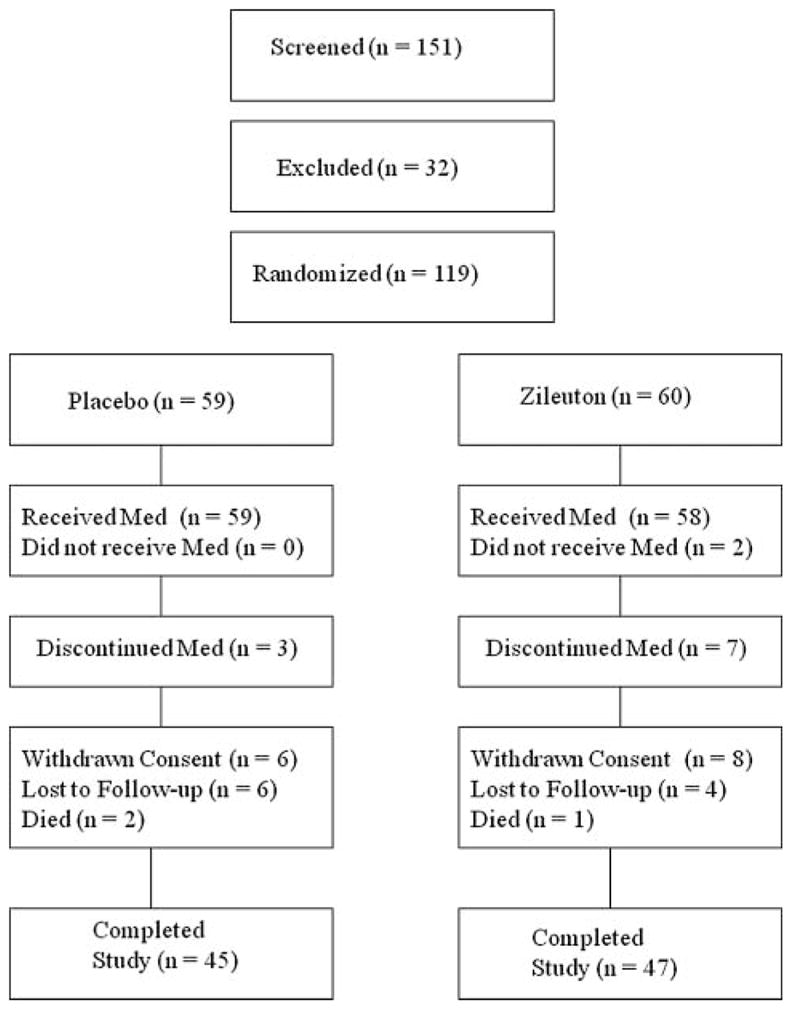
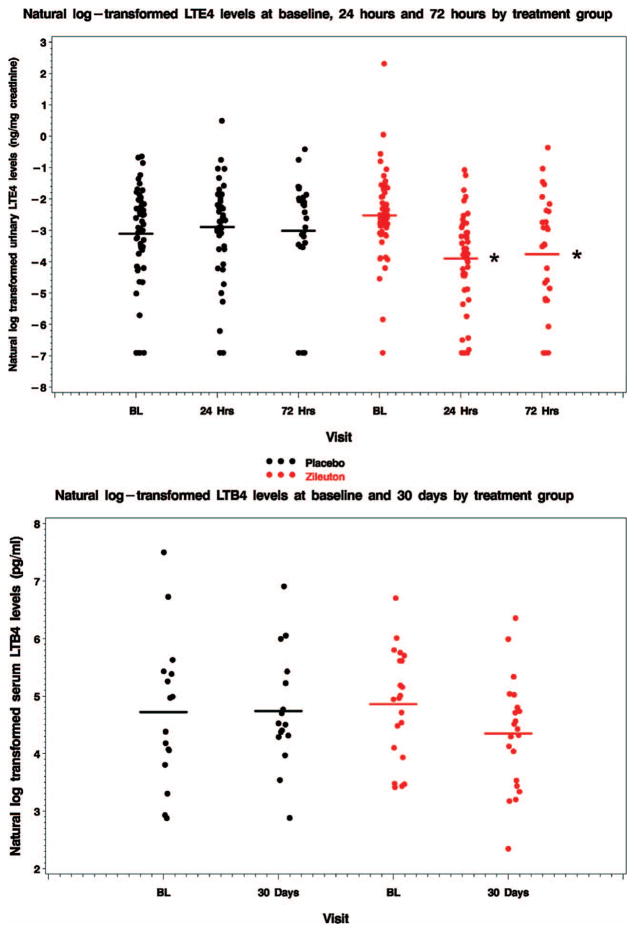
Main findings: Sixty subjects were randomized to zileuton and 59 to placebo (the study was stopped short of enrollment goals because of slow recruitment). There was no difference in hospital length of stay (3.75 +/- 2.19 vs. 3.86 +/- 3.06 days for zileuton vs. placebo, p = 0.39) or treatment failure (23% vs. 27% for zileuton vs. placebo, p = 0.63) despite a decline in urinary LTE(4) levels in the zileuton-treated group as compared to placebo at 24 hours (change in natural log-transformed ng/mg creatinine -1.38 +/- 1.19 vs. 0.14 +/- 1.51, p < 0.0001) and 72 hours (-1.32 +/- 2.08 vs. 0.26 +/- 1.93, p<0.006). Adverse events were similar in both groups.
Principal conclusions: While oral zileuton during COPD exacerbations that require hospital admission is safe and reduces urinary LTE(4) levels, we found no evidence suggesting that this intervention shortened hospital stay, with the limitation that our sample size may have been insufficient to detect a modest but potentially meaningful clinical improvement.
Trial registration: ClinicalTrials.gov NCT00493974.
Conflict of interest statement
SMS received a grant of $90,000 from Forrest Laboratories; JLC $10,001–$50,001 in capitation for a clinical trial from Boehringer Ingelheim; DEN received honoraria or advisory fees from Boehringer Ingelheim, Pfizer, AstraZeneca, GlaxoSmithKline, Nycomed, Forest Research Institute, Adams Respiratory Therapeutics, and Sepracor within the past 3 years. MTD has served on advisory boards and as a speaker for GlaxoSmithKline (<$10,000 in 2009) and Boehringer Ingelheim (<$5000 in 2009). He has received contracted research support from Aeris, Allegro, Altana/Nycomed/Forest, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Pfizer, and Roche. GJC Grant support: GlaxoSmithKline, Boehringer Ingelheim, Novartis, Respironics, Forest. Advisory groups: Dey, Boehringer Ingelheim, GlaxoSmithKline; MKH received Lecture Fees: GlaxoSmithKline, CSL Behring, Boehringer Ingelheim, Pfizer. Consulting: Novartis, Nycomed.
FJM has received speaking, consultancy and steering committee fees from GlaxoSmithKline and Nycomed. He has received speaking and consulting fees from Medimmune/Astra Zeneca, Boehringer Ingelheim (BI) and Schering. He has received consulting and steering committee fees from Actelion. He has received consulting and DSMB fees from Novartis. He has received consulting fees from Forest/Almirall, Roche, Bayer and HLS. He has received advisory board fees from Merck, Pearl, UBC, Mpex, Talecris, Comgenix, and Boom-Comm. He has received lecture fees from France Foundation, NACE, MedEd, Potomac, fb Communications, Pfizer, Vox Medic, the American Lung Association, WebMD, epocrates and HIT Global. He has received royalities from Associates in Medical Marketing, and Castle Connolly. He has received sponsored grants from the NIH. His institution has received sponsored grants from BI.
Figures

References
-
- Mannino DM, Homa DM, Akinbami LJ, Ford ES, Redd SC. MMWR Surveillance Summary No 51. CDC; 2002. Chronic Obstructive Pulmonary Disease Surveillance—United States, 1971–2002; p. SS06. - PubMed
-
- Merrill CT, Elixhauser A. 2005 HCUP Fact Book No 6. Rockville, MD: Agency for Healthcare Research and Quality; AHRQ; 2005. Hospitalization in the United States, 2002. No. 05-0056.
-
- Peters-Golden M. Expanding roles for leukotrienes in airway inflammation. Curr Allergy Asthma Rep. 2008;8(4):367–373. - PubMed
-
- Shindo K, Hirai Y, Fukumura M, Koide K. Plasma levels of leukotriene E4 during clinical course of chronic obstructive pulmonary disease. Prostaglandins Leukot Essent Fatty Acids. 1997;56(3):213–217. - PubMed
-
- Hill AT, Campbell EJ, Bayley DL, Hill SL, Stockley RA. Evidence for excessive bronchial inflammation during an acute exacerbation of chronic obstructive pulmonary disease in patients with alpha(1)-antitrypsin deficiency (PiZ) Am J Respir Crit Care Med. 1999;160(6):1968–1975. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U10 HL074416/HL/NHLBI NIH HHS/United States
- U10 HL074424/HL/NHLBI NIH HHS/United States
- UL1 TR000005/TR/NCATS NIH HHS/United States
- M01 RR000056/RR/NCRR NIH HHS/United States
- U10 HL074428/HL/NHLBI NIH HHS/United States
- U10 HL074439/HL/NHLBI NIH HHS/United States
- U10 HL074422/HL/NHLBI NIH HHS/United States
- M01 RR000425/RR/NCRR NIH HHS/United States
- U10 HL074409/HL/NHLBI NIH HHS/United States
- U10 HL074431/HL/NHLBI NIH HHS/United States
- M01 RR002635/RR/NCRR NIH HHS/United States
- U10 HL074408/HL/NHLBI NIH HHS/United States
- M01 RR000051/RR/NCRR NIH HHS/United States
- U10 HL074407/HL/NHLBI NIH HHS/United States
- M01 RR016500/RR/NCRR NIH HHS/United States
- U10 HL074441/HL/NHLBI NIH HHS/United States
- U10HL074424/HL/NHLBI NIH HHS/United States
- U10HL074428/HL/NHLBI NIH HHS/United States
- U10 HL074418/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical