

Twelve years' detection of respiratory viruses by immunofluorescence in hospitalised children: impact of the introduction of a new respiratory picornavirus assay
- PMID: 21299840
- PMCID: PMC3044667
- DOI: 10.1186/1471-2334-11-41
Twelve years' detection of respiratory viruses by immunofluorescence in hospitalised children: impact of the introduction of a new respiratory picornavirus assay
Abstract
Background: Direct immunofluorescence assays (DFA) are a rapid and inexpensive method for the detection of respiratory viruses and may therefore be used for surveillance. Few epidemiological studies have been published based solely on DFA and none included respiratory picornaviruses and human metapneumovirus (hMPV). We wished to evaluate the use of DFA for epidemiological studies with a long-term observation of respiratory viruses that includes both respiratory picornaviruses and hMPV.
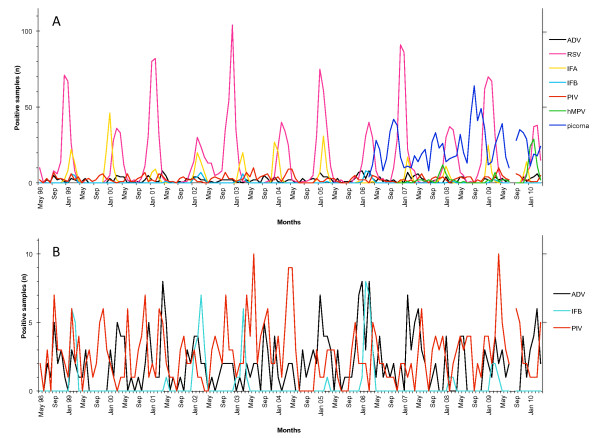
Methods: Since 1998 all children hospitalized with respiratory illness at the University Hospital Bern have been screened with DFA for common respiratory viruses including adenovirus, respiratory syncytial virus (RSV), influenza A and B, and parainfluenza virus 1-3. In 2006 assays for respiratory picornaviruses and hMPV were added. Here we describe the epidemiological pattern for these respiratory viruses detected by DFA in 10'629 nasopharyngeal aspirates collected from 8'285 patients during a 12-year period (1998-2010).
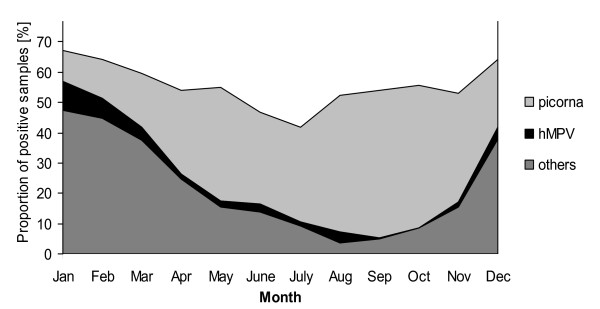
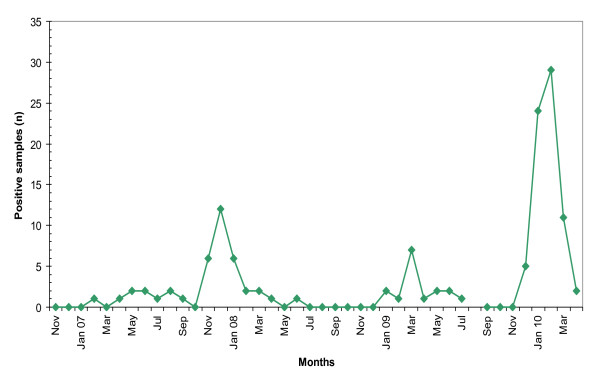
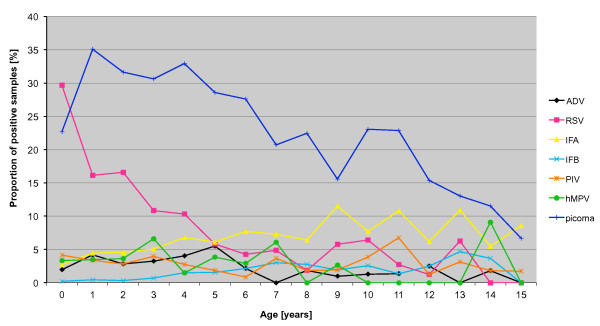
Results: Addition of assays for respiratory picornaviruses and hMPV raised the proportion of positive DFA results from 35% to 58% (p < 0.0001). Respiratory picornaviruses were the most common viruses detected among patients ≥ 1 year old. The seasonal patterns and age distribution for the studied viruses agreed well with those reported in the literature. In 2010, an hMPV epidemic of unexpected size was observed.
Conclusions: DFA is a valid, rapid, flexible and inexpensive method. The addition of assays for respiratory picornaviruses and hMPV broadens its range of viral detection. DFA is, even in the "PCR era", a particularly adapted method for the long term surveillance of respiratory viruses in a pediatric population.
Figures
References
-
- Hon KL, Nelson EA. Gender disparity in paediatric hospital admissions. Ann Acad Med Singapore. 2006;35(12):882–888. - PubMed
