

Conventional versus automated measurement of blood pressure in primary care patients with systolic hypertension: randomised parallel design controlled trial
- PMID: 21300709
- PMCID: PMC3034423
- DOI: 10.1136/bmj.d286
Conventional versus automated measurement of blood pressure in primary care patients with systolic hypertension: randomised parallel design controlled trial
Abstract
Objective: To compare the quality and accuracy of manual office blood pressure and automated office blood pressure using the awake ambulatory blood pressure as a gold standard.
Design: Multi-site cluster randomised controlled trial.
Setting: Primary care practices in five cities in eastern Canada.
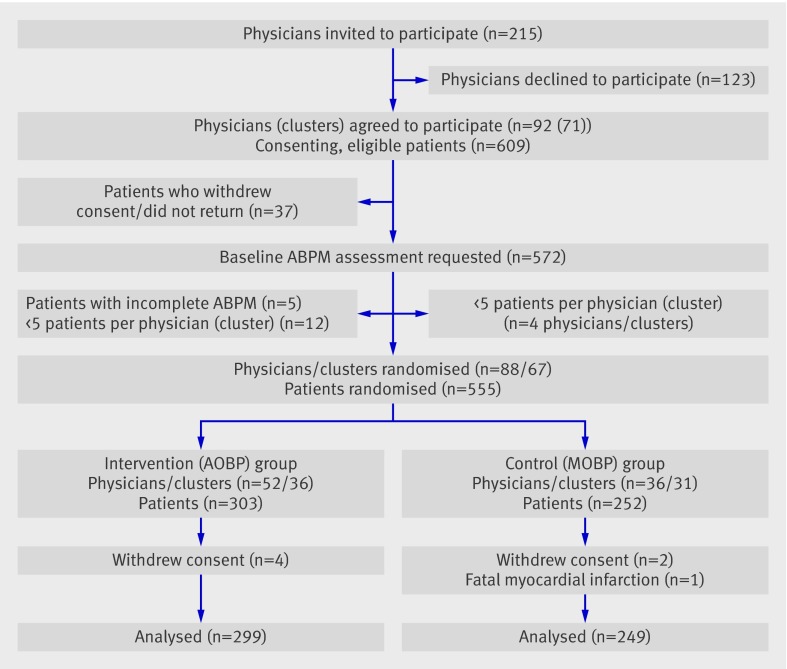
Participants: 555 patients with systolic hypertension and no serious comorbidities under the care of 88 primary care physicians in 67 practices in the community.
Interventions: Practices were randomly allocated to either ongoing use of manual office blood pressure (control group) or automated office blood pressure (intervention group) using the BpTRU device. The last routine manual office blood pressure (mm Hg) was obtained from each patient's medical record before enrollment. Office blood pressure readings were compared before and after enrollment in the intervention and control groups; all readings were also compared with the awake ambulatory blood pressure.
Main outcome measure: Difference in systolic blood pressure between awake ambulatory blood pressure minus automated office blood pressure and awake ambulatory blood pressure minus manual office blood pressure.
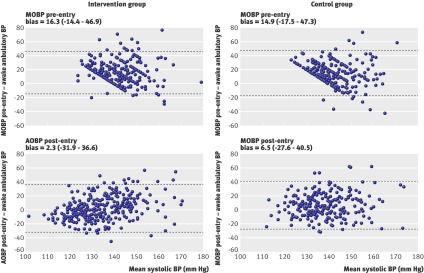
Results: Cluster randomisation allocated 31 practices (252 patients) to manual office blood pressure and 36 practices (303 patients) to automated office blood pressure measurement. The most recent routine manual office blood pressure (149.5 (SD 10.8)/81.4 (8.3)) was higher than automated office blood pressure (135.6 (17.3)/77.7 (10.9)) (P < 0.001). In the control group, routine manual office blood pressure before enrollment (149.9 (10.7)/81.8 (8.5)) was reduced to 141.4 (14.6)/80.2 (9.5) after enrollment (P < 0.001/P = 0.01), but the reduction in the intervention group from manual office to automated office blood pressure was significantly greater (P < 0.001/P = 0.02). On the first study visit after enrollment, the estimated mean difference for the intervention group between the awake ambulatory systolic/diastolic blood pressure and automated office blood pressure (-2.3 (95% confidence interval -0.31 to -4.3)/-3.3 (-2.7 to -4.4)) was less (P = 0.006/P = 0.26) than the difference in the control group between the awake ambulatory blood pressure and the manual office blood pressure (-6.5 (-4.3 to -8.6)/-4.3 (-2.9 to -5.8)). Systolic/diastolic automated office blood pressure showed a stronger (P < 0.001) within group correlation (r = 0.34/r = 0.56) with awake ambulatory blood pressure after enrollment compared with manual office blood pressure versus awake ambulatory blood pressure before enrollment (r = 0.10/r = 0.40); the mean difference in r was 0.24 (0.12 to 0.36)/0.16 (0.07 to 0.25)). The between group correlation comparing diastolic automated office blood pressure and awake ambulatory blood pressure (r = 0.56) was stronger (P < 0.001) than that for manual office blood pressure versus awake ambulatory blood pressure (r = 0.30); the mean difference in r was 0.26 (0.09 to 0.41). Digit preference with readings ending in zero was substantially reduced by use of automated office blood pressure.
Conclusion: In compliant, otherwise healthy, primary care patients with systolic hypertension, introduction of automated office blood pressure into routine primary care significantly reduced the white coat response compared with the ongoing use of manual office blood pressure measurement. The quality and accuracy of automated office blood pressure in relation to the awake ambulatory blood pressure was also significantly better when compared with manual office blood pressure. Trial registration Clinical trials NCT 00214053.
Trial registration: ClinicalTrials.gov NCT00214053.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Measurement of blood pressure in primary care.BMJ. 2011 Feb 7;342:d382. doi: 10.1136/bmj.d382. BMJ. 2011. PMID: 21300710 No abstract available.
-
Blood pressure measurement. Oscillometric devices are good in routine practice.BMJ. 2011 Mar 1;342:d1297. doi: 10.1136/bmj.d1297. BMJ. 2011. PMID: 21363844 No abstract available.
-
Hypertension: white-coat hypertension in the primary-care setting reduced with automated BP measures.Nat Rev Cardiol. 2011 Apr;8(4):184. doi: 10.1038/nrcardio.2011.33. Nat Rev Cardiol. 2011. PMID: 21553721 No abstract available.
-
Automated blood pressure readings in primary care demonstrate better correlation to the gold standard of ambulatory monitoring than manual assessment.Evid Based Med. 2011 Dec;16(6):172-3. doi: 10.1136/ebm1414. Epub 2011 Aug 4. Evid Based Med. 2011. PMID: 21816870 No abstract available.
References
-
- Pickering TG, Hall JE, Appel LJ, Falkner BE, Graves J, Hill MN, et al. Recommendations for blood pressure measurement in humans and experimental animals part 1: blood pressure measurement in humans—a statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Hypertension 2005;45:142-61. - PubMed
-
- Myers MG, Godwin M, Dawes M, Kiss A, Tobe S, Kaczorowski J. Measurement of blood pressure in the office—recognizing the problem and proposing the solution. Hypertension 2010;55:195-200. - PubMed
-
- Reeves RA. Does this patient have hypertension? How to measure blood pressure. JAMA 1995;273:1211-6. - PubMed
-
- Sala C, Santin A, Rescaldani M, Magrini F. How long shall the patient rest before clinic blood pressure measurement? Am J Hypertens 2006;19:713-7. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical