

Comparison of radiation exposure and associated radiation-induced cancer risks from mammography and molecular imaging of the breast
- PMID: 21302775
- PMCID: PMC2997811
- DOI: 10.1118/1.3512759
Comparison of radiation exposure and associated radiation-induced cancer risks from mammography and molecular imaging of the breast
Abstract
Purpose: Recent studies have raised concerns about exposure to low-dose ionizing radiation from medical imaging procedures. Little has been published regarding the relative exposure and risks associated with breast imaging techniques such as breast specific gamma imaging (BSGI), molecular breast imaging (MBI), or positron emission mammography (PEM). The purpose of this article was to estimate and compare the risks of radiation-induced cancer from mammography and techniques such as PEM, BSGI, and MBI in a screening environment.
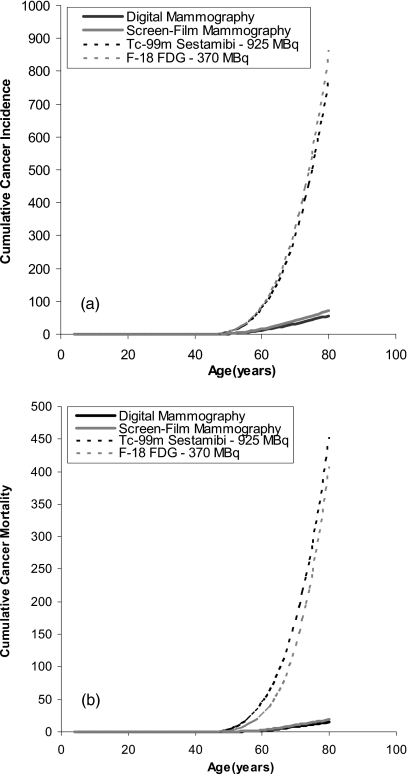
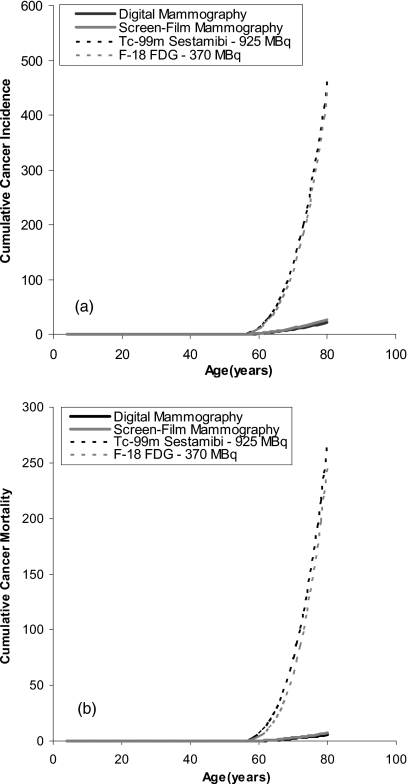
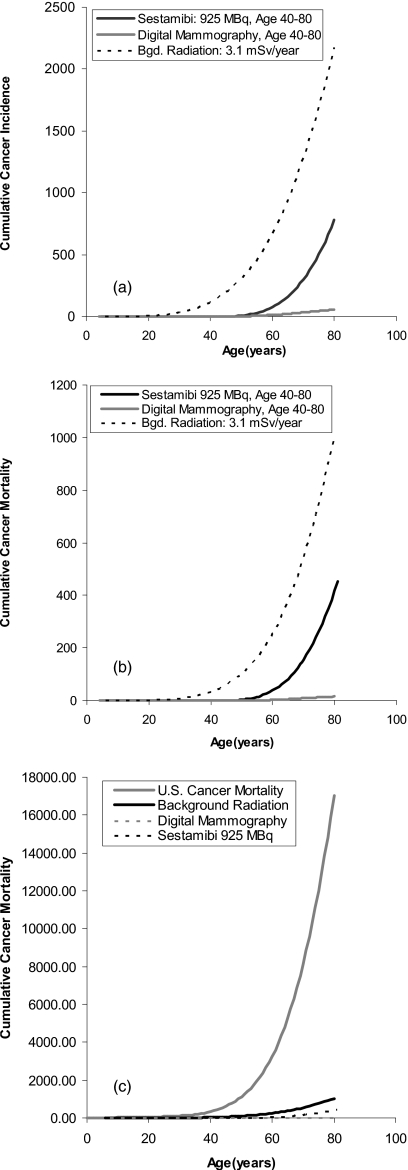
Methods: The authors used a common scheme for all estimates of cancer incidence and mortality based on the excess absolute risk model from the BEIR VII report. The lifetime attributable risk model was used to estimate the lifetime risk of radiation-induced breast cancer incidence and mortality. All estimates of cancer incidence and mortality were based on a population of 100 000 females followed from birth to age 80 and adjusted for the fraction that survives to various ages between 0 and 80. Assuming annual screening from ages 40 to 80 and from ages 50 to 80, the cumulative cancer incidence and mortality attributed to digital mammography, screen-film mammography, MBI, BSGI, and PEM was calculated. The corresponding cancer incidence and mortality from natural background radiation was calculated as a useful reference. Assuming a 15%-32% reduction in mortality from screening, the benefit/risk ratio for the different imaging modalities was evaluated.
Results: Using conventional doses of 925 MBq Tc-99m sestamibi for MBI and BSGI and 370 MBq F-18 FDG for PEM, the cumulative cancer incidence and mortality were found to be 15-30 times higher than digital mammography. The benefit/risk ratio for annual digital mammography was >50:1 for both the 40-80 and 50-80 screening groups, but dropped to 3:1 for the 40-49 age group. If the primary use of MBI, BSGI, and PEM is in women with dense breast tissue, then the administered doses need to be in the range 75-150 MBq for Tc-99m sestamibi and 35 MBq-70 MBq for F-18 FDG in order to obtain benefit/risk ratios comparable to those of mammography in these age groups. These dose ranges should be achievable with enhancements to current technology while maintaining a reasonable examination time.
Conclusions: The results of the dose estimates in this study clearly indicate that if molecular imaging techniques are to be of value in screening for breast cancer, then the administered doses need to be substantially reduced to better match the effective doses of mammography.
Figures
Similar articles
-
Radiation doses and cancer risks from breast imaging studies.Radiology. 2010 Oct;257(1):246-53. doi: 10.1148/radiol.10100570. Epub 2010 Aug 24. Radiology. 2010. PMID: 20736332 Review.
-
Benefit to Radiation Risk of Breast-specific Gamma Imaging Compared with Mammography in Screening Asymptomatic Women with Dense Breasts.Radiology. 2016 Nov;281(2):583-588. doi: 10.1148/radiol.2016151581. Epub 2016 Jun 3. Radiology. 2016. PMID: 27257949
-
Radiation Doses and Risks in Breast Screening.J Breast Imaging. 2020 Jun 3;2(3):188-200. doi: 10.1093/jbi/wbaa016. J Breast Imaging. 2020. PMID: 38424982
-
Radiation-Induced Breast Cancer Incidence and Mortality From Digital Mammography Screening: A Modeling Study.Ann Intern Med. 2016 Feb 16;164(4):205-14. doi: 10.7326/M15-1241. Epub 2016 Jan 12. Ann Intern Med. 2016. PMID: 26756460 Free PMC article.
-
Mammography-oncogenecity at low doses.J Radiol Prot. 2009 Jun;29(2A):A123-32. doi: 10.1088/0952-4746/29/2A/S08. Epub 2009 May 19. J Radiol Prot. 2009. PMID: 19454801 Review.
Cited by
-
Proof of concept for low-dose molecular breast imaging with a dual-head CZT gamma camera. Part I. Evaluation in phantoms.Med Phys. 2012 Jun;39(6):3466-75. doi: 10.1118/1.4718665. Med Phys. 2012. PMID: 22755726 Free PMC article.
-
The Impact of Reduced Injected Radioactivity on Image Quality of Molecular Breast Imaging Tomosynthesis.Breast Imaging (2012). 2012 Jul;7361:300-307. doi: 10.1007/978-3-642-31271-7_39. Breast Imaging (2012). 2012. PMID: 28835942 Free PMC article.
-
Dedicated Breast Gamma Camera Imaging and Breast PET: Current Status and Future Directions.PET Clin. 2018 Jul;13(3):363-381. doi: 10.1016/j.cpet.2018.02.008. PET Clin. 2018. PMID: 30100076 Free PMC article. Review.
-
Proof of concept for low-dose molecular breast imaging with a dual-head CZT gamma camera. Part II. Evaluation in patients.Med Phys. 2012 Jun;39(6):3476-83. doi: 10.1118/1.4719959. Med Phys. 2012. PMID: 22755727 Free PMC article.
-
Radiology's Ionising Radiation Paradox: Weighing the Indispensable Against the Detrimental in Medical Imaging.Cureus. 2023 Jul 10;15(7):e41623. doi: 10.7759/cureus.41623. eCollection 2023 Jul. Cureus. 2023. PMID: 37435015 Free PMC article. Review.
References
-
- Lee C. H. et al., “Breast cancer screening with imaging: Recommendations from the society of breast imaging and the ACR on the use of mammography, breast MRI, breast ultrasound, and other technologies for the detection of clinically occult breast cancer,” J. Am. Coll. Radiol. ZZZZZZ 7, 18–27 (2010).10.1016/j.jacr.2009.09.022 - DOI - PubMed
-
- Carney P. A. et al., “Individual and combined effects of age, breast density, and hormone replacement therapy use on the accuracy of screening mammography,” Ann. Intern Med. ZZZZZZ 138, 168–175 (2003). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
