

Use of a continuous glucose sensor in an extracorporeal life support circuit
- PMID: 21303630
- PMCID: PMC3045226
- DOI: 10.1177/193229681100500113
Use of a continuous glucose sensor in an extracorporeal life support circuit
Abstract
Background: Standard care for infants on extracorporeal life support (ECLS) relies on intermittent measurement of blood glucose (BG); however, this can lead to significant changes in BG that go unrecognized for several hours. The present study was designed to assess performance and clinical applicability of a subcutaneous glucose sensor technology modified for use as a blood-contacting sensor within the ECLS circuit.
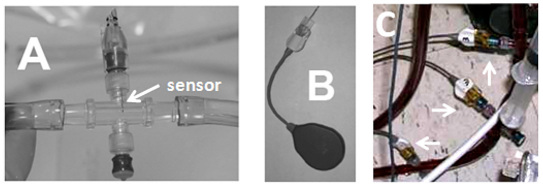
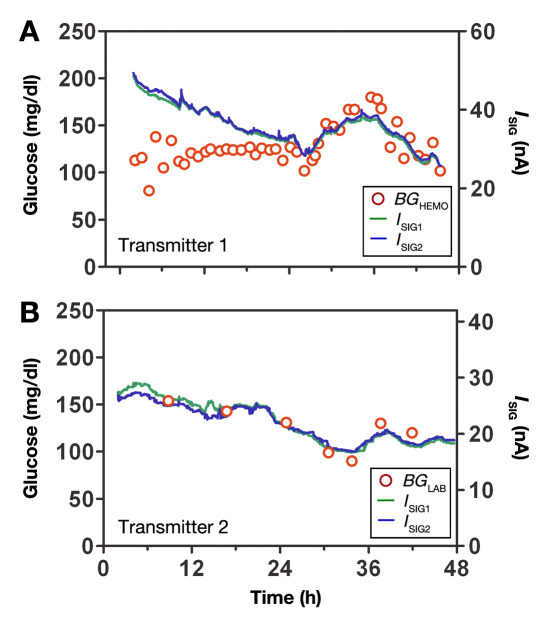
Methods: Twelve children, aged 3 years or less, requiring ECLS support were studied. Three continuous glucose sensors (Medtronic MiniMed) were inserted into hubs placed in line with the ECLS circuit. Blood glucose was assessed with a laboratory analyzer (BG(LAB); Bayer Rapidlab 860) approximately every 5 h (mean 4.9 ± 3.3 h) with more frequent samples obtained with a bedside monitor (HemoCue) as needed. Sensor current (I(SIG)) was transmitted to a laptop computer and retrospectively calibrated using BGLAB. Sensor performance was assessed by mean absolute relative difference (MARD), linear regression slope and intercept, and correlation, all with BGLAB as reference.
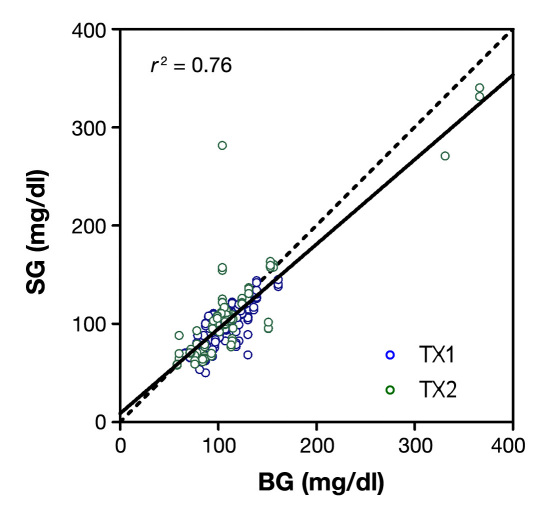
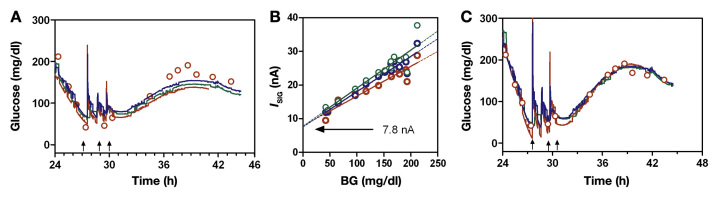
Results: The BGLAB averaged 107.6 ± 36.4 mg/dl (mean ± standard deviation) ranging from 58 to 366 mg/dl. The MARD was 11.4%, with linear regression slope (0.86 ± 0.030) and intercept (9.0 ± 3.2 mg/dl) different from 1 and 0, respectively (p < .05), and correlation (r² = 0.76; p < .001). The system was not associated with any adverse events, and placement and removal into the hubs was easily accomplished. Instances in which more frequent BG values were obtained using a bedside HemoCue (BGHEMO) monitor showed the sensor to respond rapidly to changes.
Conclusions: We conclude that continuous sensors can be adapted for use in an ECLS circuit with accuracy similar to or better than that achieved with the subcutaneous site. Continuous glucose monitoring in this population can rapidly detect changes in BG that would not otherwise be observed. Further studies will be needed to assess the benefit of continuous glucose monitoring in this population.
© 2010 Diabetes Technology Society.
Figures
Similar articles
-
Performance evaluation of three continuous glucose monitoring systems: comparison of six sensors per subject in parallel.J Diabetes Sci Technol. 2013 Jul 1;7(4):842-53. doi: 10.1177/193229681300700406. J Diabetes Sci Technol. 2013. PMID: 23911165 Free PMC article. Clinical Trial.
-
Rate-of-Change Dependence of the Performance of Two CGM Systems During Induced Glucose Swings.J Diabetes Sci Technol. 2015 Jul;9(4):801-7. doi: 10.1177/1932296815578716. Epub 2015 Apr 7. J Diabetes Sci Technol. 2015. PMID: 25852074 Free PMC article.
-
The first use of live continuous glucose monitoring in patients on extracorporeal life support.Diabetes Technol Ther. 2005 Jun;7(3):431-9. doi: 10.1089/dia.2005.7.431. Diabetes Technol Ther. 2005. PMID: 15929674
-
Current status of pediatric/neonatal extracorporeal life support: clinical outcomes, circuit evolution, and translational research.Perfusion. 2011 Jul;26(4):294-301. doi: 10.1177/0267659111401673. Epub 2011 Feb 28. Perfusion. 2011. PMID: 21357633 Review.
-
Accuracy of Freestyle Libre continuous glucose monitoring system in critically ill patients after cardiac surgery.J Cardiothorac Surg. 2025 Jan 20;20(1):75. doi: 10.1186/s13019-024-03229-1. J Cardiothorac Surg. 2025. PMID: 39833920 Free PMC article. Review.
Cited by
-
Fear of Self-Injecting and Self-Testing and the Related Risk Factors in Adolescents with Type 1 Diabetes: A Cross-Sectional Study.Diabetes Ther. 2017 Feb;8(1):75-83. doi: 10.1007/s13300-016-0221-8. Epub 2016 Dec 19. Diabetes Ther. 2017. PMID: 27995595 Free PMC article.
-
The artificial pancreas: evaluating risk of hypoglycaemia following errors that can be expected with prolonged at-home use.Diabet Med. 2016 Feb;33(2):235-42. doi: 10.1111/dme.12823. Epub 2015 Jul 4. Diabet Med. 2016. PMID: 26036309 Free PMC article.
-
Hypoglycemia in critically ill children.J Diabetes Sci Technol. 2012 Jan 1;6(1):48-57. doi: 10.1177/193229681200600107. J Diabetes Sci Technol. 2012. PMID: 22401322 Free PMC article.
References
-
- Conrad SA, Rycus PT, Dalton H. Extracorporeal Life Support Registry Report 2004. ASAIO J. 2005;51(1):4–10. - PubMed
-
- Kyle UG, Jolliet P, Genton L, Meier CA, Mensi N, Graf JD, Chevrolet JC, Pichard C. Clinical evaluation of hormonal stress state in medical ICU patients: a prospective blinded observational study. Intensive Care Med. 2005;31(12):1669–1675. - PubMed
-
- Glass P, Wagner AE, Papero PH, Rajasingham SR, Civitello LA, Kjaer MS, Coffman CE, Getson PR, Short BL. Neurodevelopmental status at age five years of neonates treated with extracorporeal membrane oxygenation. J Pediatr. 1995;127(3):447–457. - PubMed
-
- Short BL. The effect of extracorporeal life support on the braa focus on ECMO. Semin Perinatol. 2005;29(1):45–50. - PubMed
-
- Renard E, Costalat G, Chevassus H, Bringer J. Artificial beta-cell: clinical experience toward an implantable closed-loop insulin delivery system. Diabetes Metab. 2006;32(5 Pt 2):497–502. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
