

Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: a randomized clinical trial
- PMID: 21304082
- PMCID: PMC5389857
- DOI: 10.1001/jama.2011.90
Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: a randomized clinical trial
Abstract
Context: Sentinel lymph node dissection (SLND) accurately identifies nodal metastasis of early breast cancer, but it is not clear whether further nodal dissection affects survival.
Objective: To determine the effects of complete axillary lymph node dissection (ALND) on survival of patients with sentinel lymph node (SLN) metastasis of breast cancer.
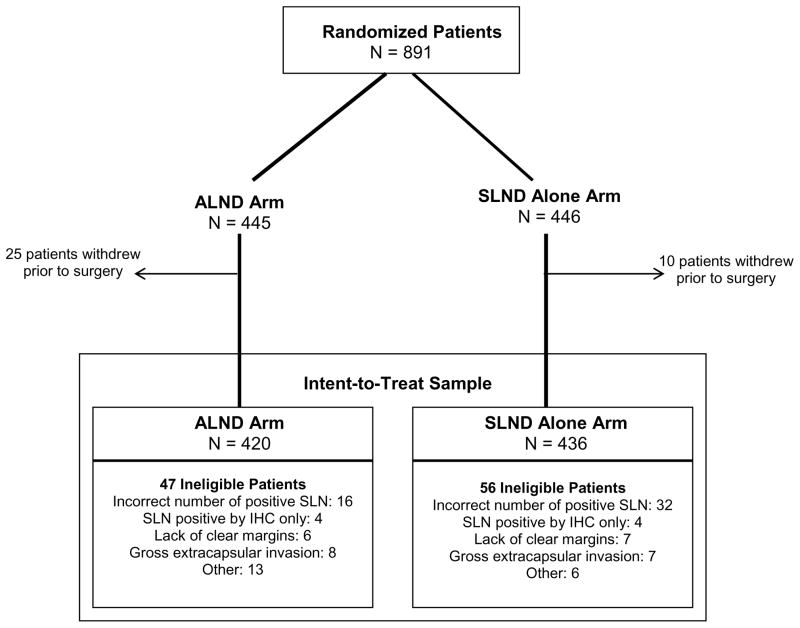
Design, setting, and patients: The American College of Surgeons Oncology Group Z0011 trial, a phase 3 noninferiority trial conducted at 115 sites and enrolling patients from May 1999 to December 2004. Patients were women with clinical T1-T2 invasive breast cancer, no palpable adenopathy, and 1 to 2 SLNs containing metastases identified by frozen section, touch preparation, or hematoxylin-eosin staining on permanent section. Targeted enrollment was 1900 women with final analysis after 500 deaths, but the trial closed early because mortality rate was lower than expected.
Interventions: All patients underwent lumpectomy and tangential whole-breast irradiation. Those with SLN metastases identified by SLND were randomized to undergo ALND or no further axillary treatment. Those randomized to ALND underwent dissection of 10 or more nodes. Systemic therapy was at the discretion of the treating physician.
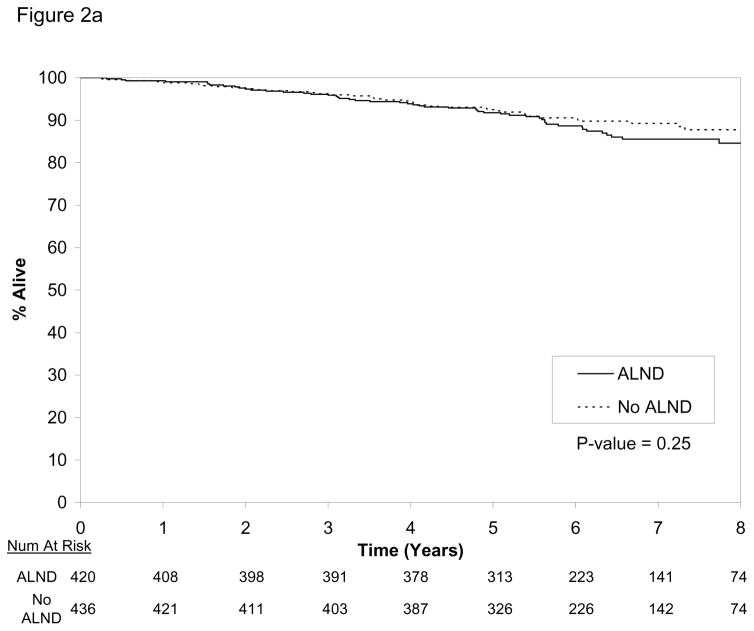
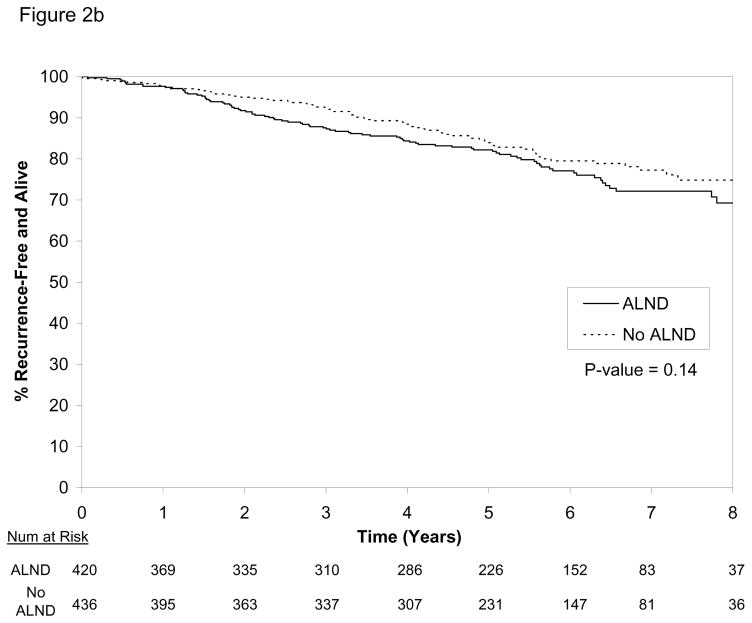
Main outcome measures: Overall survival was the primary end point, with a noninferiority margin of a 1-sided hazard ratio of less than 1.3 indicating that SLND alone is noninferior to ALND. Disease-free survival was a secondary end point.
Results: Clinical and tumor characteristics were similar between 445 patients randomized to ALND and 446 randomized to SLND alone. However, the median number of nodes removed was 17 with ALND and 2 with SLND alone. At a median follow-up of 6.3 years (last follow-up, March 4, 2010), 5-year overall survival was 91.8% (95% confidence interval [CI], 89.1%-94.5%) with ALND and 92.5% (95% CI, 90.0%-95.1%) with SLND alone; 5-year disease-free survival was 82.2% (95% CI, 78.3%-86.3%) with ALND and 83.9% (95% CI, 80.2%-87.9%) with SLND alone. The hazard ratio for treatment-related overall survival was 0.79 (90% CI, 0.56-1.11) without adjustment and 0.87 (90% CI, 0.62-1.23) after adjusting for age and adjuvant therapy.
Conclusion: Among patients with limited SLN metastatic breast cancer treated with breast conservation and systemic therapy, the use of SLND alone compared with ALND did not result in inferior survival.
Trial registration: clinicaltrials.gov Identifier: NCT00003855.
Conflict of interest statement
The authors indicate no potential conflicts of interest.
Figures
Comment in
-
Management of axillary lymph node metastasis in breast cancer: making progress.JAMA. 2011 Feb 9;305(6):606-7. doi: 10.1001/jama.2011.131. JAMA. 2011. PMID: 21304087 No abstract available.
-
Axillary vs sentinel lymph node dissection for invasive breast cancer.JAMA. 2011 Jun 8;305(22):2288-9; author reply 2290-1. doi: 10.1001/jama.2011.751. JAMA. 2011. PMID: 21642671 No abstract available.
-
Axillary vs sentinel lymph node dissection for invasive breast cancer.JAMA. 2011 Jun 8;305(22):2288; author reply 2290-1. doi: 10.1001/jama.2011.750. JAMA. 2011. PMID: 21642672 No abstract available.
-
Axillary vs sentinel lymph node dissection for invasive breast cancer.JAMA. 2011 Jun 8;305(22):2289; author reply 2290-1. doi: 10.1001/jama.2011.753. JAMA. 2011. PMID: 21642673 No abstract available.
-
Axillary vs sentinel lymph node dissection for invasive breast cancer.JAMA. 2011 Jun 8;305(22):2289; author reply 2290-1. doi: 10.1001/jama.2011.752. JAMA. 2011. PMID: 21642674 No abstract available.
-
Axillary vs sentinel lymph node dissection for invasive breast cancer.JAMA. 2011 Jun 8;305(22):2290; author reply 2290-1. doi: 10.1001/jama.2011.755. JAMA. 2011. PMID: 21642675 No abstract available.
-
Axillary vs sentinel lymph node dissection for invasive breast cancer.JAMA. 2011 Jun 8;305(22):2290; author reply 2290-1. doi: 10.1001/jama.2011.754. JAMA. 2011. PMID: 21642676 No abstract available.
-
Omitting axilla lymphadenectomy even by positive sentinel lymph node: a change in breast cancer treatment practice.Womens Health (Lond). 2011 Jul;7(4):417-8. doi: 10.2217/whe.11.46. Womens Health (Lond). 2011. PMID: 21790334
-
Less may be better: axillary dissection is unnecessary in some patients with a positive sentinel lymph node.Arch Surg. 2011 Aug;146(8):980-2. doi: 10.1001/archsurg.2011.181. Arch Surg. 2011. PMID: 21844441 No abstract available.
-
CAGS and ACS Evidence Based Reviews in Surgery. 40. Axillary dissection versus no axillary dissection in women with invasive breast cancer and sentinel node metastasis.Can J Surg. 2012 Feb;55(1):66-9. doi: 10.1503/cjs.036011. Can J Surg. 2012. PMID: 22269305 Free PMC article. No abstract available.
-
[Axillary dissection vs. no axillary dissection in women with invasive breast cancer and sentinel node metastasis: implications for the radiation oncologist].Strahlenther Onkol. 2012 Dec;188(12):1155-6. doi: 10.1007/s00066-012-0247-4. Strahlenther Onkol. 2012. PMID: 23135733 German. No abstract available.
References
-
- Fisher B, Wolmark N, Bauer M, Redmond C, Gebhardt M. The accuracy of clinical nodal staging and of limited axillary dissection as a determinant of histologic nodal status in carcinoma of the breast. Surg Gynecol Obstet. 1981 Jun;152(6):765–772. - PubMed
-
- Graversen HP, Blichert-Toft M, Andersen JA, Zedeler K. Breast cancer: risk of axillary recurrence in node-negative patients following partial dissection of the axilla. Eur J Surg Oncol. 1988 Oct;14(5):407–412. - PubMed
-
- Fisher B, Jeong JH, Anderson S, Bryant J, Fisher ER, Wolmark N. Twenty-five-year follow-up of a randomized trial comparing radical mastectomy, total mastectomy, and total mastectomy followed by irradiation. N Engl J Med. 2002 Aug 22;347(8):567–575. - PubMed
-
- Orr RK. The impact of prophylactic axillary node dissection on breast cancer survival--a Bayesian meta-analysis. Ann Surg Oncol. 1999 Jan-Feb;6(1):109–116. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
