

The association of left ventricular hypertrophy with metabolic syndrome is dependent on body mass index in hypertensive overweight or obese patients
- PMID: 21304952
- PMCID: PMC3031611
- DOI: 10.1371/journal.pone.0016630
The association of left ventricular hypertrophy with metabolic syndrome is dependent on body mass index in hypertensive overweight or obese patients
Abstract
Background: Overweight (Ow) and obesity (Ob) influence blood pressure (BP) and left ventricular hypertrophy (LVH). It is unclear whether the presence of metabolic syndrome (MetS) independently affects echocardiographic parameters in hypertension.
Methods: 380 Ow/Ob essential hypertensive patients (age ≤ 65 years) presenting for referred BP control-related problems. MetS was defined according to NCEP III/ATP with AHA modifications and LVH as LVM/h(2.7) ≥ 49.2 g/m(2.7) in males and ≥ 46.7 g/m(2.7) in females. Treatment intensity score (TIS) was used to control for BP treatment as previously reported.
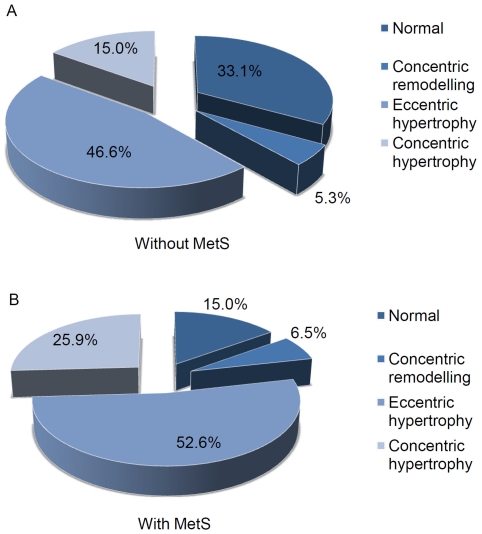
Results: Hypertensive patients with MetS had significantly higher BMI, systolic and mean BP, interventricular septum and relative wall thickness and lower ejection fraction than those without MetS. LVM/h(2.7) was significantly higher in MetS patients (59.14 ± 14.97 vs. 55.33 ± 14.69 g/m(2.7); p = 0.022). Hypertensive patients with MetS had a 2.3-fold higher risk to have LVH/h(2.7) after adjustment for age, SBP and TIS (OR 2.34; 95%CI 1.40-3.92; p = 0.001), but MetS lost its independent relationship with LVH when BMI was included in the model.
Conclusions: In Ow/Ob hypertensive patients MetS maintains its role of risk factor for LVH independently of age, SBP, and TIS, resulting in a useful predictor of target organ damage in clinical practice. However, MetS loses its independent relationship when BMI is taken into account, suggesting that the effects on MetS on LV parameters are mainly driven by the degree of adiposity.
Conflict of interest statement
Figures
References
-
- Poirier P, Giles TD, Bray GA, Hong Y, Stern JS, et al. American Heart Association; Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. Obesity and cardiovascular disease: pathophysiology, evaluation, and effect of weight loss: an update of the 1997 American Heart Association Scientific Statement on Obesity and Heart Disease from the Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. Circulation. 2006;113:898–918. - PubMed
-
- MacMahon S, Alderman MH, Lindholm LH, Liu L, Sanchez RA, et al. Blood-pressure-related disease is a global health priority. Lancet. 2008;371:1480–1482. - PubMed
-
- Cutler JA, Sorlie PD, Wolz M, Thom T, Fields LE, et al. Trends in Hypertension Prevalence, Awareness, Treatment, and Control Rates in United States Adults Between 1988-1994 and 1999-2004. Hypertension. 2008;52:818–827. - PubMed
-
- Krauser DG, Devereux RB. Ventricular hypertrophy and hypertension: prognostic elements and implications for management. Herz. 2006;31:305–16. - PubMed
-
- Schillaci G, Verdecchia P, Porcellati C, Cuccurullo O, Cosco C, et al. Continuous relation between left ventricular mass and cardiovascular risk in essential hypertension. Hypertension. 2000;35:580–586. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
