

Retinal redox stress and remodeling in cardiometabolic syndrome and diabetes
- PMID: 21307645
- PMCID: PMC3154050
- DOI: 10.4161/oxim.3.6.14786
Retinal redox stress and remodeling in cardiometabolic syndrome and diabetes
Abstract
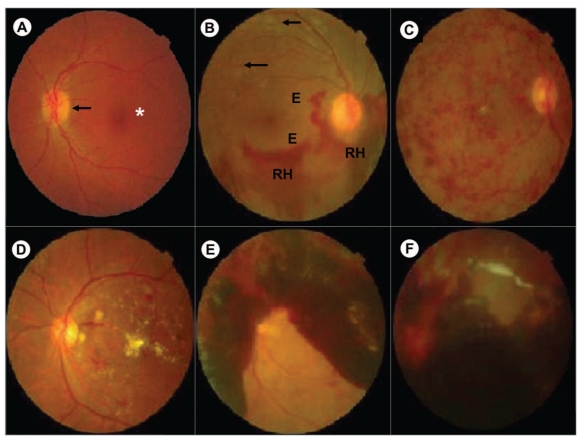
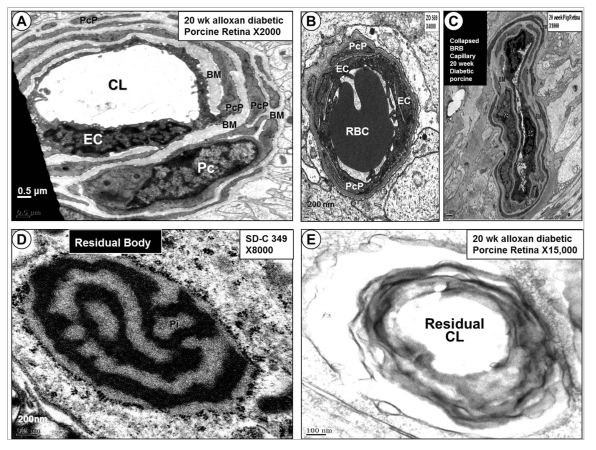
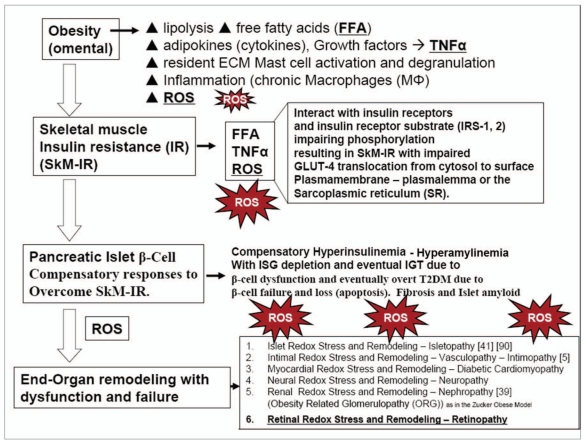
Diabetic retinopathy (DR) is a significant cause of global blindness; a major cause of blindness in the United States in people aged between 20-74. There is emerging evidence that retinopathy is initiated and propagated by multiple metabolic toxicities associated with excess production of reactive oxygen species (ROS). The four traditional metabolic pathways involved in the development of DR include: increased polyol pathway flux, advanced glycation end-product formation, activation of protein kinase C isoforms, and hexosamine pathway flux. These pathways individually and synergistically contribute to redox stress with excess ROS resulting in retinal tissue injury resulting in significant microvascular blood retinal barrier remodeling. The toxicity of hyperinsulinemia, hyperglycemia, hypertension, dyslipidemia, increased cytokines and growth factors, in conjunction with redox stress, contribute to the development and progression of DR. Redox stress contributes to the development and progression of abnormalities of endothelial cells and pericytes in DR. This review focuses on the ultrastructural observations of the blood retinal barrier including the relationship between the endothelial cell and pericyte remodeling in young nine week old Zucker obese (fa/fa) rat model of obesity; cardiometabolic syndrome, and the 20 week old alloxan induced diabetic porcine model. Preventing or delaying the blindness associated with these intersecting abnormal metabolic pathways may be approached through strategies targeted to reduction of tissue inflammation and oxidative - redox stress. Understanding these abnormal metabolic pathways and the accompanying redox stress and remodeling may provide both the clinician and researcher a new concept of approaching this complicated disease process.
Figures





References
-
- Wong TY, Duncan BB, Golden SH, et al. Associations between the metabolic syndrome and retinal microvascular signs: the atherosclerosis risk in communities study. Investigative Ophthalmology and Visual Science. 2004;45(9):2949–2954. - PubMed
-
- Serne EH, Ijzerman RG, de Jongh RT, Stehouwer CD. Blood pressure and insulin resistance: role for microvascular function? Cardiovascular Research. 2002;53:271–276. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
