

Predictors of treatment outcome in modular cognitive therapy for obsessive-compulsive disorder
- PMID: 21308884
- PMCID: PMC3076701
- DOI: 10.1002/da.20785
Predictors of treatment outcome in modular cognitive therapy for obsessive-compulsive disorder
Abstract
Background: The present study sought to identify predictors of outcome for a comprehensive cognitive therapy (CT) developed for patients with obsessive-compulsive disorder (OCD).
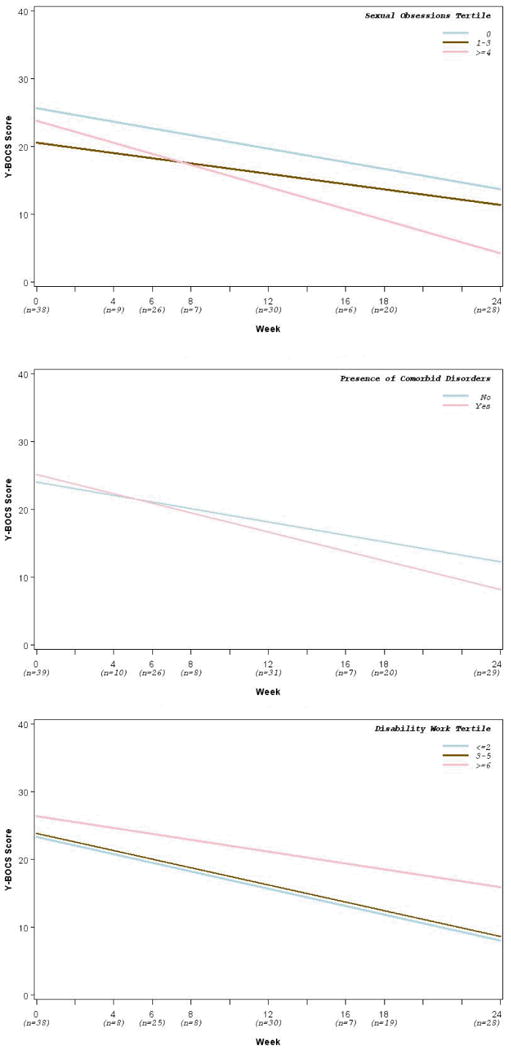
Methods: Treatment was delivered over 22 sessions and included standard CT methods, as well as specific strategies designed for subtypes of OCD including religious, sexual, and other obsessions. This study of 39 participants assigned to CT examined predictors of outcomes assessed on the Yale-Brown Obsessive Compulsive Scale. A variety of baseline symptom variables were examined as well as treatment expectancy and motivation.
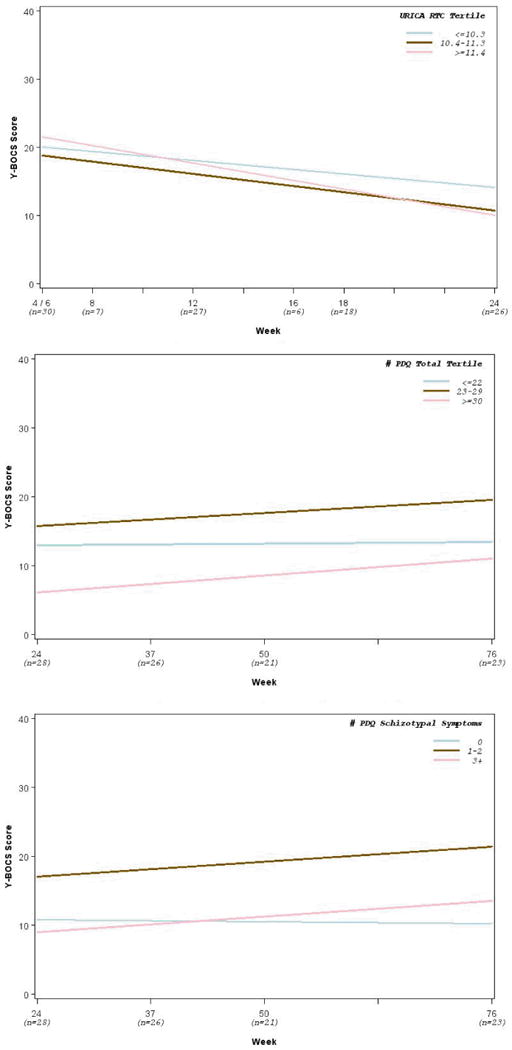
Results: Findings indicated that participants who perceived themselves as having more severe OCD at baseline remained in treatment but more severe symptoms were marginally associated with worse outcome for those who completed therapy. Depressed and anxious mood did not predict post-test outcome, but more Axis I comorbid diagnoses (mainly major depression and anxiety disorders), predicted more improvement, as did the presence of sexual (but not religious) OCD symptoms, and stronger motivation (but not expectancy). A small rebound in OCD symptoms at 1-year follow-up was significantly predicted by higher scores on personality traits, especially for schizotypal (but not obsessive-compulsive personality) traits.
Conclusions: Longer treatment may be needed for those with more severe symptoms at the outset. CT may have positive effects not only on OCD symptoms but also on comorbid depressive and anxious disorders and associated underlying core beliefs. Findings are discussed in light of study limitations and research on other predictors.
© 2011 Wiley-Liss, Inc.
Figures
Similar articles
-
Treatment of obsessive-compulsive disorder in patients who have comorbid major depression.J Clin Psychol. 2004 Nov;60(11):1133-41. doi: 10.1002/jclp.20078. J Clin Psychol. 2004. PMID: 15389622
-
Clinical predictors of long-term outcome in obsessive-compulsive disorder.Depress Anxiety. 2013 Aug;30(8):763-72. doi: 10.1002/da.22013. Epub 2012 Oct 25. Depress Anxiety. 2013. PMID: 23109056 Clinical Trial.
-
Social skills training in a case of obsessive-compulsive disorder with schizotypal personality disorder.J Behav Ther Exp Psychiatry. 1996 Jun;27(2):189-94. doi: 10.1016/0005-7916(96)00010-9. J Behav Ther Exp Psychiatry. 1996. PMID: 8894918
-
Personality disorders in obsessive compulsive disorder.Psychiatr Clin North Am. 1992 Dec;15(4):803-12. Psychiatr Clin North Am. 1992. PMID: 1461797 Review.
-
Schizotypal personality disorder in clinical obsessive-compulsive disorder samples: a brief overview.CNS Spectr. 2021 Oct;26(5):468-480. doi: 10.1017/S1092852920001716. Epub 2020 Jul 27. CNS Spectr. 2021. PMID: 32713392 Review.
Cited by
-
Predictors of response to cognitive behaviour therapy for obsessive-compulsive disorder.Int J Clin Health Psychol. 2015 Sep-Dec;15(3):181-190. doi: 10.1016/j.ijchp.2015.07.003. Epub 2015 Aug 10. Int J Clin Health Psychol. 2015. PMID: 30487835 Free PMC article.
-
The cognitive model of negative symptoms: a systematic review and meta-analysis of the dysfunctional belief systems associated with negative symptoms in schizophrenia spectrum disorders.Psychol Med. 2025 Feb 5;55:e11. doi: 10.1017/S0033291724003325. Psychol Med. 2025. PMID: 39905754 Free PMC article.
-
Determining prognostic variables of treatment outcome in obsessive-compulsive disorder: effectiveness and its predictors in routine clinical care.Eur Arch Psychiatry Clin Neurosci. 2022 Mar;272(2):313-326. doi: 10.1007/s00406-021-01284-6. Epub 2021 Jul 3. Eur Arch Psychiatry Clin Neurosci. 2022. PMID: 34218306 Free PMC article.
-
Predictors and moderators of symptom change during cognitive-behavioral therapy or supportive psychotherapy for body dysmorphic disorder.J Affect Disord. 2021 May 15;287:34-40. doi: 10.1016/j.jad.2021.03.011. Epub 2021 Mar 11. J Affect Disord. 2021. PMID: 33773357 Free PMC article. Clinical Trial.
-
An investigation of outcome expectancies as a predictor of treatment response for combat veterans with PTSD: comparison of clinician, self-report, and biological measures.Depress Anxiety. 2015 Jun;32(6):392-9. doi: 10.1002/da.22354. Epub 2015 Feb 19. Depress Anxiety. 2015. PMID: 25703611 Free PMC article. Clinical Trial.
References
-
- National Institute for Health and Clinical Excellence . Obsessive-compulsive disorder (National Clinical Practice Guideline 31) London, UK: The British Psychological Society & The Royal College of Psychiatrists; 2006. Retrieved August 12, 2007, from www.nice.org.uk.
-
- Franklin ME, Abramowitz JS, Kozak MJ, et al. Effectiveness of exposure and ritual prevention for obsessive-compulsive disorder: Randomized compared with nonrandomized samples. J Consult Clin Psychol. 2000;68:594–602. - PubMed
-
- Rachman S. A cognitive theory of obsessions. Behav Res Ther. 1997;35:793–802. - PubMed
-
- Group OCCW Cognitive assessment of obsessive-compulsive disorder. Behav Res Ther. 1997;35:667–681. - PubMed
-
- Cottraux J, Note I, Yao SN, et al. A randomized controlled trial of cognitive therapy versus intensive behavior therapy in obsessive compulsive disorder. Psychother Psychosom. 2001;70:288–297. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
