

Zinc for attention-deficit/hyperactivity disorder: placebo-controlled double-blind pilot trial alone and combined with amphetamine
- PMID: 21309695
- PMCID: PMC3037197
- DOI: 10.1089/cap.2010.0073
Zinc for attention-deficit/hyperactivity disorder: placebo-controlled double-blind pilot trial alone and combined with amphetamine
Abstract
Objective: To explore effects of zinc supplementation in American children with attention-deficit/hyperactivity disorder (ADHD). Mideastern trials reported significant benefit from 13-40 mg elemental zinc as the sulfate.
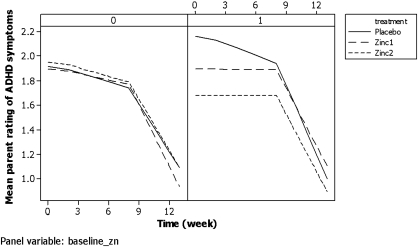
Method: We randomly assigned 52 children aged 6-14 with DSM-IV ADHD to zinc supplementation (15 mg every morning [qAM] or two times per day [b.i.d.] as glycinate, n = 28) or matched placebo (n = 24) for 13 weeks: 8 weeks monotherapy and then 5 weeks with added d-amphetamine (AMPH). AMPH dose was weight-standardized for 2 weeks and then clinically optimized by week 13. Zinc glycinate was chosen as having less gastrointestinal discomfort than sulfate. Hypotheses were that zinc would improve inattention more than placebo by effect size of d > 0.25 at 8 weeks; zinc+AMPH would improve ADHD symptoms more than placebo+AMPH by d > 0.25, and optimal dose of AMPH with zinc would be 20% lower than with placebo. An interim analysis requested by the National Institute of Mental Health resulted in an increased dosage, so that 20 received 15 mg/day qAM and 8 received 30 mg/day (15 mg b.i.d.)
Results: Only the third hypothesis was upheld: Optimal mg/kg AMPH dose with b.i.d. zinc was 37% lower than with placebo. Other clinical outcomes were equivocal, sometimes favoring zinc, sometimes placebo, but objective neuropsychological measures mostly favored b.i.d. zinc (d = 0.36-0.7). Safety tests and adverse events were not different between groups. Copper and iron blood indices were not impaired by 8 weeks of 30 mg/day zinc.
Conclusion: Doses up to 30 mg/day of zinc were safe for at least 8 weeks, but clinical effect was equivocal except for 37% reduction in amphetamine optimal dose with 30 mg/day zinc (not with 15 mg). Possible reasons for difference from mideastern reports include endemic diets, population genetics, relative rate of zinc deficiency, difference in background nutrition, insufficient dosage or absorption, or wrong anion (sulfate may be necessary for reported benefit). Dose may be especially important: All visually impressive advantages over placebo appeared only with 15 mg b.i.d. rather than once a day. Future research should use larger doses than 15 mg/day, provide a basic recommended daily allowance/intake multivitamin/mineral supplement for all to standardize background nutrition, select participants for low zinc, and consider the issue of anion interaction.
Figures
References
-
- Aman MG. Applications of computerized cognitive-motor measures to the assessment of psychoactive drugs. In: WE. Dodson., editor; M. Kinsbourne., editor; B. Hiltbrunner., editor. The Assessment of Cognitive Function in Epilepsy. New York: Demos Publications; 1991. pp. 69–96.
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Fourth. Washington, DC: American Psychiatric Association; 1994. (DSM-IV)
-
- Arnold LE. Pinkham SM. Votolato N. Does zinc moderate essential fatty acid and amphetamine treatment of attention-deficit/hyperactivity disorder? J Child Adolesc Psychopharmacol. 2000;10:111–117. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
