

Irreversible electroporation of the liver and liver hilum in swine
- PMID: 21309933
- PMCID: PMC3048967
- DOI: 10.1111/j.1477-2574.2010.00261.x
Irreversible electroporation of the liver and liver hilum in swine
Abstract
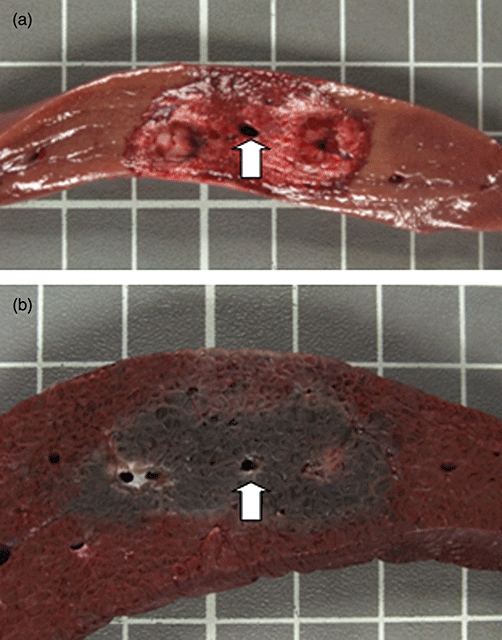
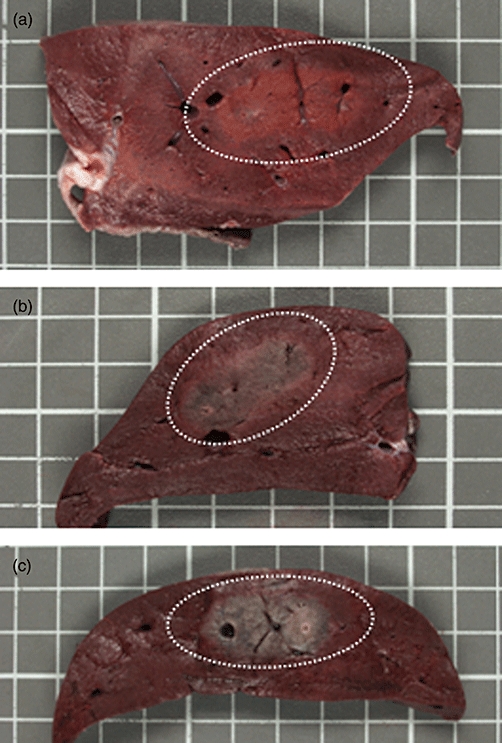
Background: Irreversible electroporation (IRE) is a novel, non-thermal form of ablation. We studied the safety and efficacy of IRE for the ablation of liver tissue around the liver hilum. We also studied the ability of triphenyltetrazolium chloride staining (TTC) to predict the zone of ablation after IRE.
Methods: Eight swine underwent 20 ablations of the liver and liver hilum. Two monopolar probes were positioned 2 cm apart. IRE was performed using 90 pulses of 2500-3000 V/cm. IRE treatments were performed from 15 min to 14 days (n= 4) before sacrifice.
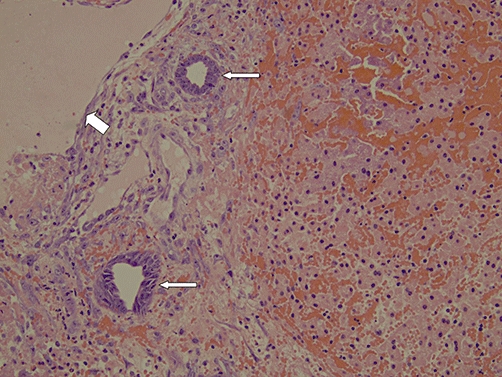
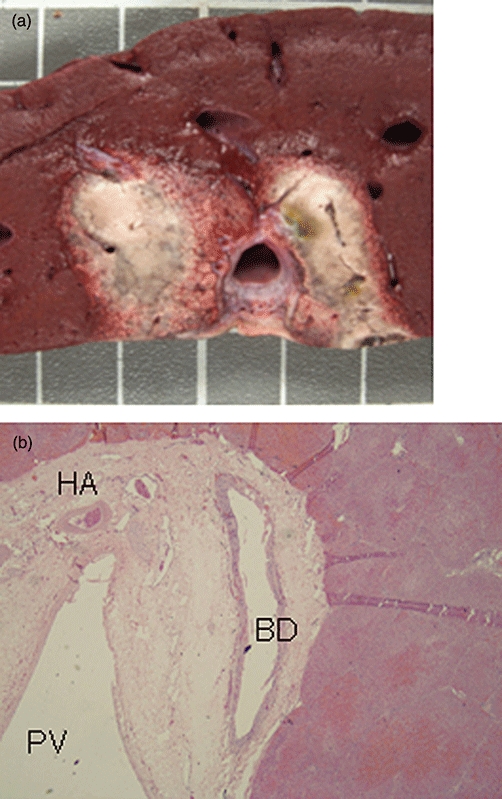
Results: All animals survived. No major complications were encountered. Ablation width ranged from 2.27 to 4.45 cm and ablation height ranged from 1.5 to 1.8 cm. TTC staining demonstrated the zone of ablation in all animals. Hepatocyte necrosis occurs immediately adjacent to large central veins without evidence of heat sink. Bile ducts, portal veins and hepatic arteries appear to be more resistant to the effects of IRE.
Conclusions: IRE appears to be safe and effective for liver tissue ablation in the liver hilum. The portal structures appear more resistant to the effects of IRE. TTC staining can predict the zone of IRE ablation as early as 15 min after treatment.
© 2011 International Hepato-Pancreato-Biliary Association.
Figures
References
-
- Pompili M, Mirante VG, Rondinara G, Fassati LR, Piscaglia F, Agnes S, et al. Percutaneous ablation procedures in cirrhotic patients with hepatocellular carcinoma submitted to liver transplantation: assessment of efficacy at explant analysis and of safety for tumor recurrence. Liver Transpl. 2005;11:1117–1126. - PubMed
-
- Shibata T, Iimuro Y, Yamamoto Y, Maetani Y, Ametani F, Itoh K, et al. Small hepatocellular carcinoma: comparison of radiofrequency ablation and percutaneous microwave coagulation therapy. Radiology. 2002;223:331–337. - PubMed
-
- Goldberg SN, Dupuy D. Image-guided radiofrequency tumor ablation: challenges and opportunities-Part I. J Vasc Interv Radiol. 2001;12:1021–1032. - PubMed
-
- Goldberg SN, Hahn PF, Tanabe KK, Mueller PR, Schima W, Athanasoulis CA, et al. Percutaneous radiofrequency tissue ablation: does perfusion-mediated tissue cooling limit coagulation necrosis? J Vasc Interv Radiol. 1998;9:101–111. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
