

Liver grafts from selected older donors do not have significantly more ischaemia reperfusion injury
- PMID: 21309940
- PMCID: PMC3048974
- DOI: 10.1111/j.1477-2574.2010.00275.x
Liver grafts from selected older donors do not have significantly more ischaemia reperfusion injury
Abstract
Background: There is a general concern that aged organs are more susceptible to ischaemia. In the light of recent proposals to change the liver allocation system by expanding regional sharing, it is feared that increased cold ischaemia time of grafts from older donors may reduce graft survival. The aim of this study was to correlate donor age and the patterns of ischaemia reperfusion injury and synthetic function early after liver transplantation.
Methods: We performed a retrospective study of first transplants using a single-centre electronic database. Patterns of liver injury (based on transaminases and post-reperfusion biopsy), synthetic function (international normalized ratio [INR]), and graft and patient survival in recipients receiving liver grafts from donors aged ≥ 65 years (group 1, n= 50) were compared with equivalent patterns in a matched cohort of recipients transplanted with grafts from donors aged <65 years (group 2, n= 50).
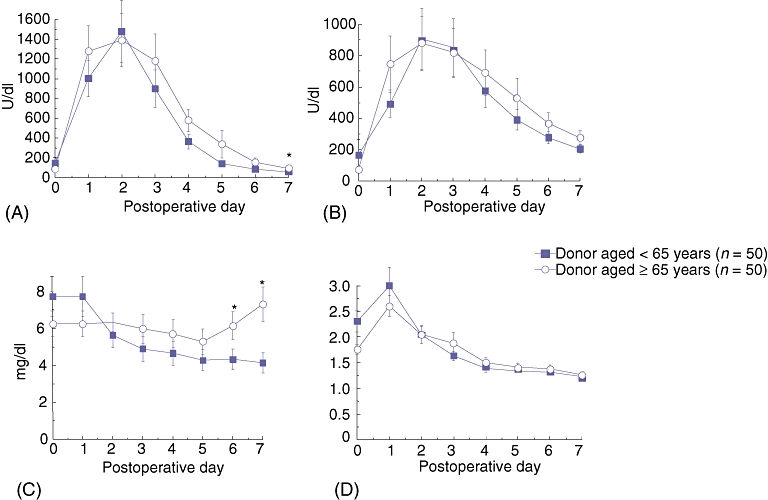
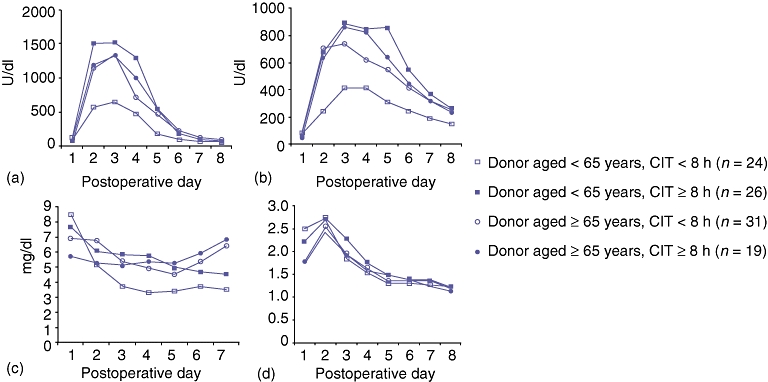
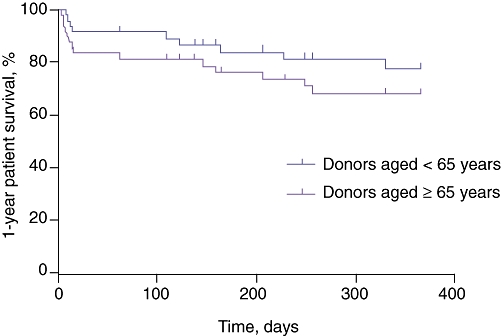
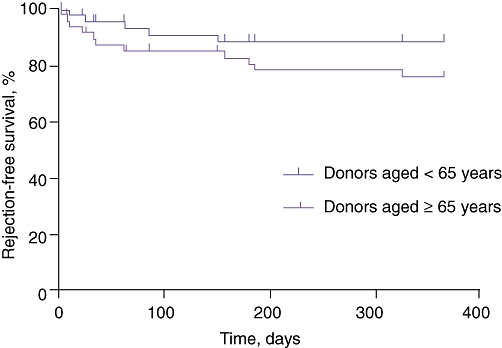
Results: There was no significant difference in transaminase levels from day 0 to day 6 after transplantation. When groups 1 and 2 were subdivided into two subgroups based on the duration of graft cold ischaemia time (<8 h and ≥ 8 h), there was no statistical difference in transaminase levels during the first 7 days. There were two cases (4%) of primary non-function in group 1 and one (2%) in group 2. Initial poor function did not differ significantly between the groups (26% vs. 24%; P= 0.81). In addition, there was no difference in histological changes in post-reperfusion biopsies (21% vs. 34%; P= 0.078) and rate of acute rejection episodes in the first year (30% vs. 32%; P= 0.99). There was no significant difference between groups 1 and 2 in 1-year patient and graft survivals (78% vs. 90% [P= 0.17]; 88% vs. 94% [P= 0.48], respectively).
Conclusions: Judiciously selected livers from aged donors are not associated with major increased susceptibility to ischaemia reperfusion injury.
© 2011 International Hepato-Pancreato-Biliary Association.
Figures
References
-
- Scientific Registry of Transplant Recipients. 2005 Annual Report of the US Organ Procurement and Transplantation Network and Scientific Registry of Transplant Recipients. 2005. Transplant data 1995–2004. http://www.ustransplant.org/annual_reports/current/. [Accessed June 2010.
-
- Ploeg RJ, D'Alessandro AM, Knechtle SJ, Stegall MD, Pirsch JD, Hoffmann RM, et al. Risk factors for primary dysfunction after liver transplantation – a multivariate analysis. Transplantation. 1993;55:807–813. - PubMed
-
- Berenguer M. Risk of extended criteria donors in hepatitis C virus-positive recipients. Liver Transpl. 2008;14(Suppl):45–50. - PubMed
-
- Strasberg SM, Howard TK, Molmenti EP, Hertl M. Selecting the donor liver: risk factors for poor function after orthotopic liver transplantation. Hepatology. 1994;20:829–838. - PubMed
-
- Mazzafero V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334:693–699. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
