

Serious infection risk and immune recovery after double-unit cord blood transplantation without antithymocyte globulin
- PMID: 21310254
- PMCID: PMC3165093
- DOI: 10.1016/j.bbmt.2011.02.001
Serious infection risk and immune recovery after double-unit cord blood transplantation without antithymocyte globulin
Abstract
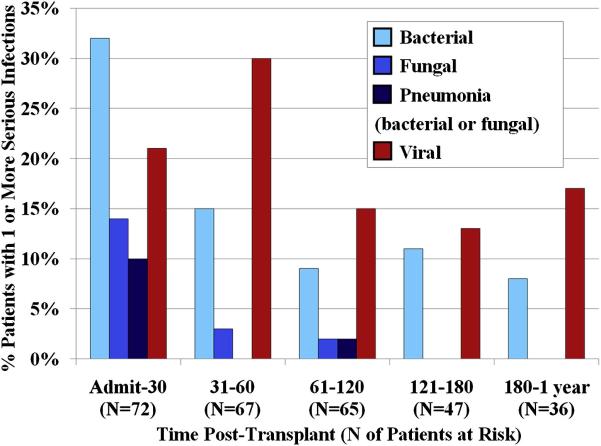
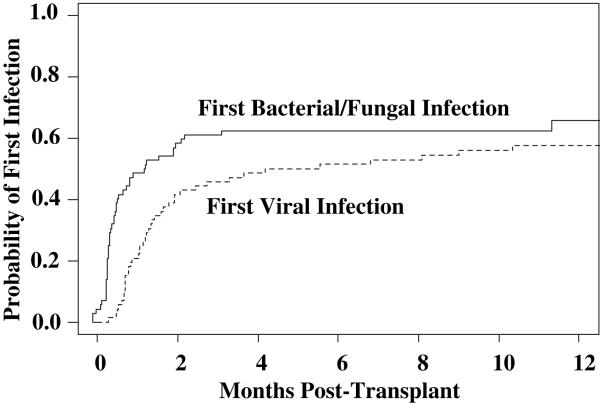
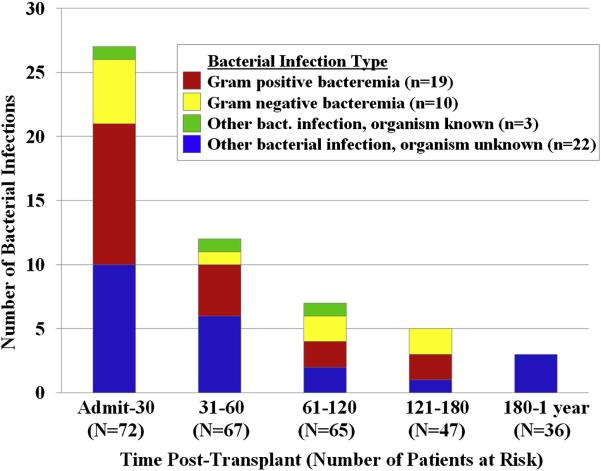
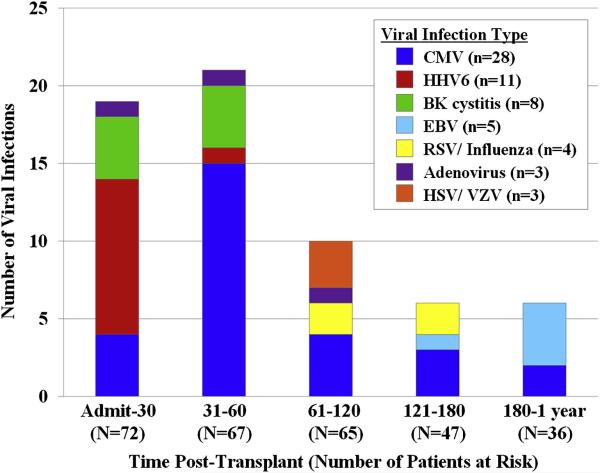
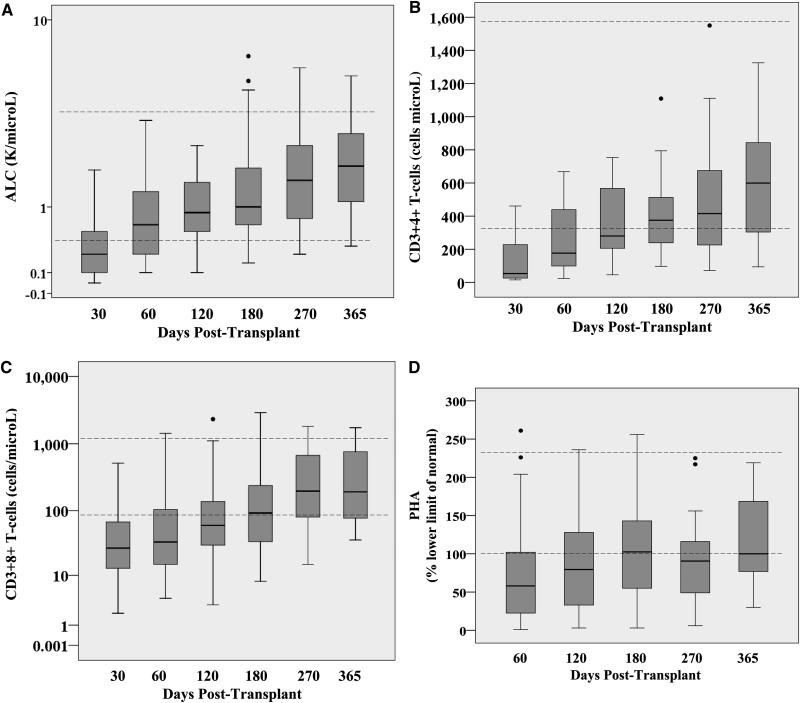
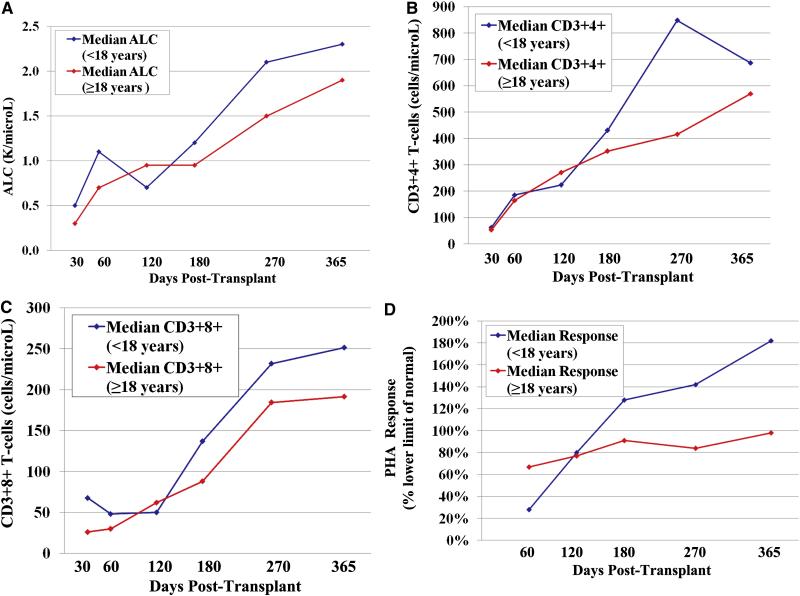
Factors contributing to infection risk after cord blood transplantation (CBT) include the use of anti-thymocyte globulin (ATG), prolonged neutropenia, and failure to transfer immunity. In the present study, we investigated the potential of double-unit CBT without ATG to reduce the risk of infection and evaluated the nature of serious infections in the first year after CBT using this approach. Seventy-two predominantly adult patients underwent CBT for hematologic malignancies; of these, 52 patients received myeloablative conditioning, and 20 received nonmyeloablative conditioning. The peak incidences of bacterial infections (32%), fungal infections (14%), and bacterial/fungal pneumonias (10%) occurred in the first 30 days posttransplantation. Three such infections contributed to early mortality. The peak incidence of viral infections was 31-60 days posttransplantation, affecting 30% of patients. Cytomegalovirus (CMV) was the most common viral infection. CMV infections occurring before day 120 (n = 23) had no relationship with graft-versus-host disease (GVHD), whereas CMV infections occurring after day 120 (n = 5), along with all cases of Epstein-Barr virus viremia (n = 5) and adenoviral enteritis (n = 2), occurred exclusively in the context of GVHD therapy or corticosteroid use for another indication. Viral infections had the highest lethality: 2 were a direct cause of death, and 3 contributed to death. Patients exhibited steady immune recovery, achieving a median CD3(+)4(+) T cell count >200 cells/μL by day 120 post-CBT, and no infection-related deaths occurred after day 120. Our results suggest that double-unit CBT without ATG is associated with prompt T cell recovery, and, unlike in CBT incorporating ATG, infection is rarely a primary cause of death. However, CBT without ATG is associated with a significant risk of GVHD, and serious infections remain a challenge, especially in the setting of GVHD. New strategies are needed to further reduce infectious complications after CBT; these will require earlier neutrophil recovery and more effective prevention of GVHD, ideally without the profound T cell depletion associated with ATG therapy.
Copyright © 2011 American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Barker JN, Weisdorf DJ, DeFor TE, et al. Transplantation of two partially HLA-matched umbilical cord blood units to enhance engraftment in adults with hematologic malignancy. Blood. 2005;105:1343–1347. - PubMed
-
- Michallet M, Ito JI. Approaches to the management of invasive fungal infections in hematologic malignancy and hematopoietic cell transplantation. J Clin Oncol. 2009;27:3398–3409. - PubMed
-
- Cohen J, Gandhi M, Naik P, et al. Increased incidence of EBV-related disease following paediatric stem cell transplantation with reduced-intensity conditioning. Br J Haematol. 2005;129:229–239. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
