

Case Reports
doi: 10.3174/ajnr.A2349.
Epub 2011 Feb 10.
Complex spinal-paraspinal fast-flow lesions in CLOVES syndrome: analysis of clinical and imaging findings in 6 patients
Affiliations
- PMID: 21310861
- PMCID: PMC7966001
- DOI: 10.3174/ajnr.A2349
Item in Clipboard
Case Reports
Complex spinal-paraspinal fast-flow lesions in CLOVES syndrome: analysis of clinical and imaging findings in 6 patients
AJNR Am J Neuroradiol.
2011 Nov-Dec.
Abstract
CLOVES syndrome is a complex disorder of congenital lipomatous overgrowth, vascular malformations, epidermal nevi, and skeletal/scoliosis/spinal anomalies. We report the occurrence of spinal-paraspinal fast-flow lesions within or adjacent to the truncal overgrowth or a cutaneous birthmark in 6 patients with CLOVES syndrome.
Figures
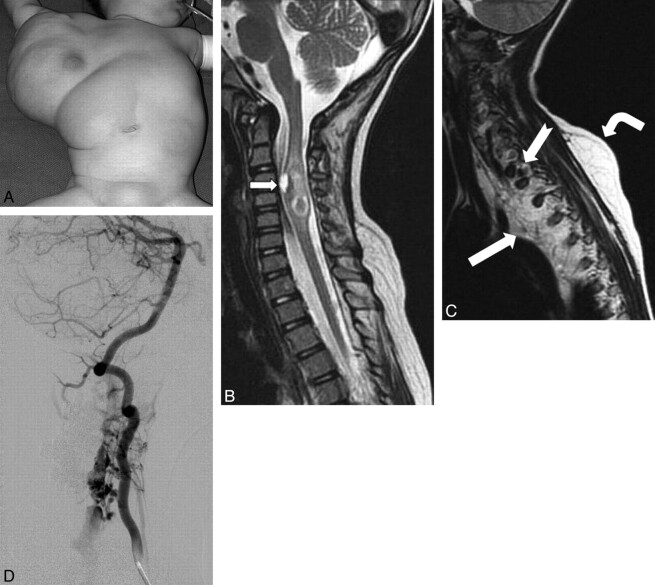
A, Frontal photograph before the first surgical debulking. A large truncal mass extends into the right axilla, chest, and upper abdominal walls. Note a faint capillary malformation overlying the mass. B, Sagittal T2 MR image of the cervicothoracic spine demonstrates an expansile heterogeneous intramedullary lesion within the cervical spinal cord from the C4 to C6 levels, with signal-intensity characteristics consistent with blood products. A ventral cord lesion demonstrates a fluid-fluid level indicating an acute parenchymal hematoma (arrow). Perilesional T2 hyperintense rim is consistent with edema. C, Sagittal T2 MR image shows a diffuse involvement of the mediastinum and the paraspinal musculature with lymphatic malformation (white arrow) and fatty tissue, with marked deviation and compression of the spinal cord. There is an asymmetric fatty overgrowth of the spinal canal with the subcutaneous layer (bent arrow) insinuating into it via the neuroforamina, with large flow-void signals (notched arrow). D, Right vertebral arteriogram. The arterial supply to the epidural portion comes via the C3, C4, and C5 segmental branches of the right vertebral artery. The anterior and posterior spinal arteries are unremarkable. The lesion drains into markedly dilated epidural veins coursing inferiorly within the spinal canal and exits at a left upper thoracic neural foramen.
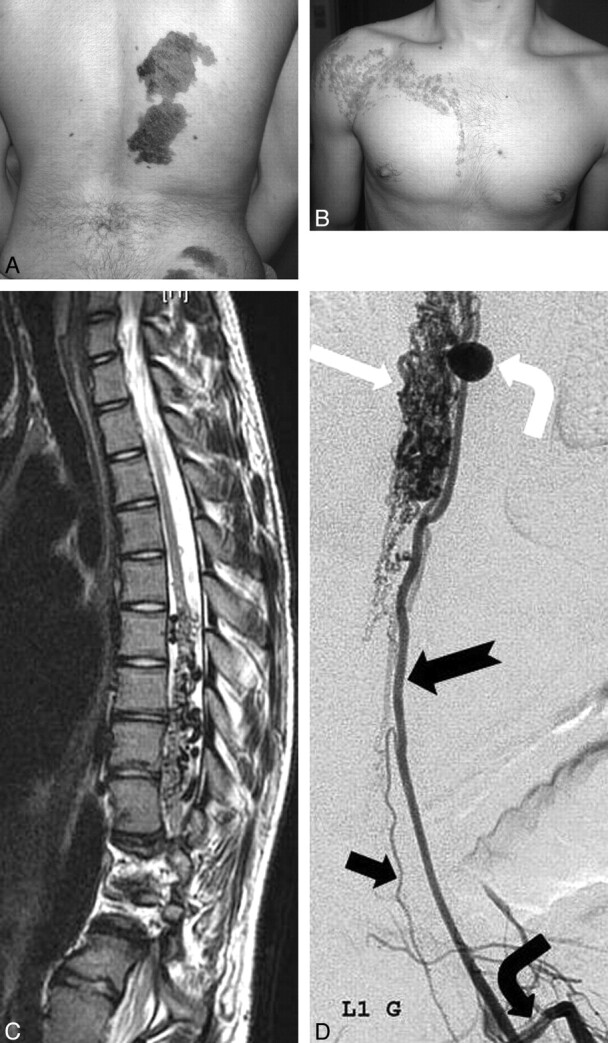
A, Multiple congenital dark nevi and capillary stains of the right paraspinal and gluteal areas. B, Linear epidermal nevus of the right shoulder and chest wall. Neither of these lesions crosses the midline. C, Spinal sagittal T2-weighted MR image demonstrates enlarged tortuous intradural flow voids (dorsally > ventrally) in the lower thoracic spine. The cord has an irregular contour due to the intradural dilated vessels, with focal hyperintense changes. Note also the extensive involvement of the adjacent vertebrae. D, Selective angiography of left first lumbar artery (bent black arrow) reveals an enlarged radiculomedullary artery (notched arrow) supplying an extensive dilated pial network (white arrow) on the surface of the cord via large pial branches. There is a large arterial aneurysm of the ascending pial branch (bent white arrow). Note the radiculomedullary supply to the anterior spinal artery (black arrow).
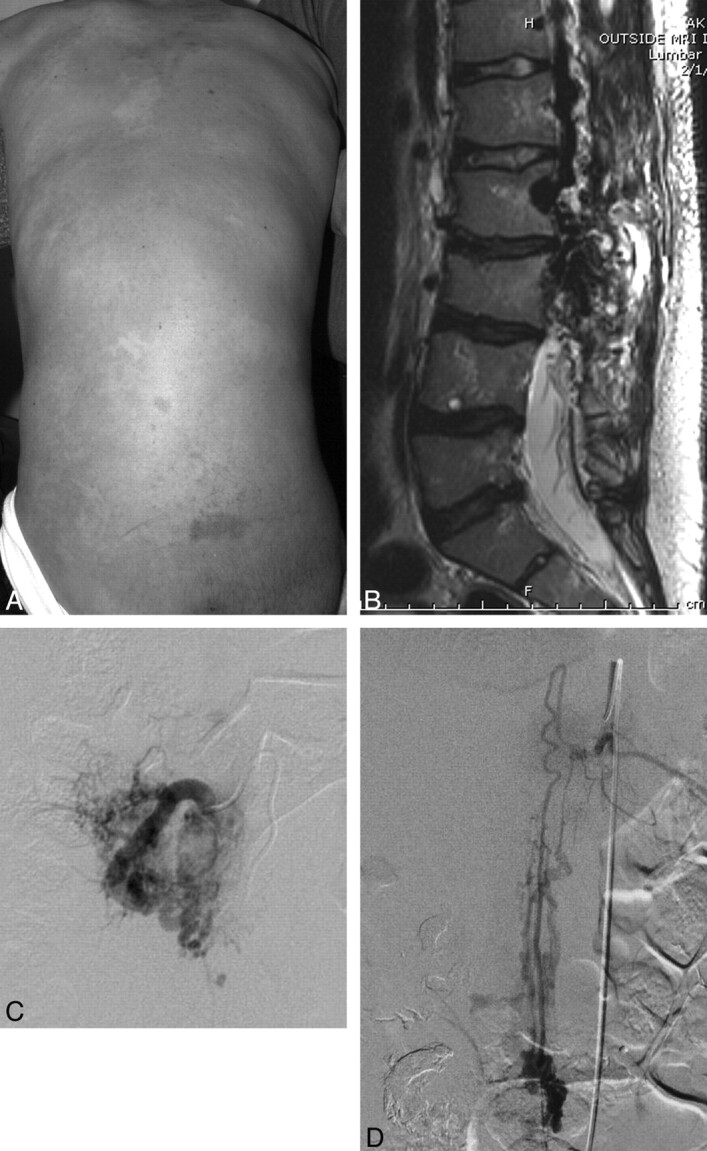
A, Faint diffuse capillary stain covering asymmetrically thickened soft tissue of the back and scoliosis. B, Sagittal T2-weighted MR image demonstrates a large area of abnormal heterogeneous tissue and signal-intensity void involving the paraspinal muscles, thecal sac, and adjacent lumbar vertebrae. Some fatty thickening and flow voids are also seen in the retroperitoneum. There is some loss of anterior height of the lumbar vertebrae with irregular contour, dehydration of the intervertebral disks, and kyphosis. C, Selective angiogram of the right L3 segmental artery demonstrates arterial dilation with extensive supply to the paravertebral AVM, centered within the paraspinal musculature. D, Selective study of the artery of Adamkiewicz (left T11) demonstrates a pial arteriovenous fistula at the L2 level.
References
-
- Biesecker LG, Happle R, Mulliken JB, et al. Proteus syndrome: diagnostic criteria, differential diagnosis, and patient evaluation. Am J Med Genet 1999;84:389–95 - PubMed
-
- Turner JT, Cohen MM, Jr,, Biesecker LG. Reassessment of the Proteus syndrome literature: application of diagnostic criteria to published cases. Am J Med Genet A 2004;130A:111–22 - PubMed
-
- Sapp JC, Turner JT, van de Kamp JM, et al. Newly delineated syndrome of congenital lipomatous overgrowth, vascular malformations, and epidermal nevi (CLOVE syndrome) in seven patients. Am J Med Genet A 2007;143A:2944–58 - PubMed
-
- Alomari AI. Characterization of a distinct syndrome that associates complex truncal overgrowth, vascular, and acral anomalies: a descriptive study of 18 cases of CLOVES syndrome. Clin Dysmorphol 2009;18:1–7 - PubMed
-
- Aminoff MJ, Logue V. The prognosis of patients with spinal vascular malformations. Brain 1974;97:211–18. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical